

Cost-effectiveness of Transforaminal epidural steroid injections for patients with ACUTE sciatica: a randomized controlled trial
- PMID: 38561748
- PMCID: PMC10983727
- DOI: 10.1186/s12891-024-07366-5
Cost-effectiveness of Transforaminal epidural steroid injections for patients with ACUTE sciatica: a randomized controlled trial
Abstract
Background: Transforaminal epidural injections with steroids (TESI) are increasingly being used in patients sciatica. The STAR (steroids against radiculopathy)-trial aimed to evaluate the (cost-) effectiveness of TESI in patients with acute sciatica (< 8 weeks). This article contains the economic evaluation of the STAR-trial.
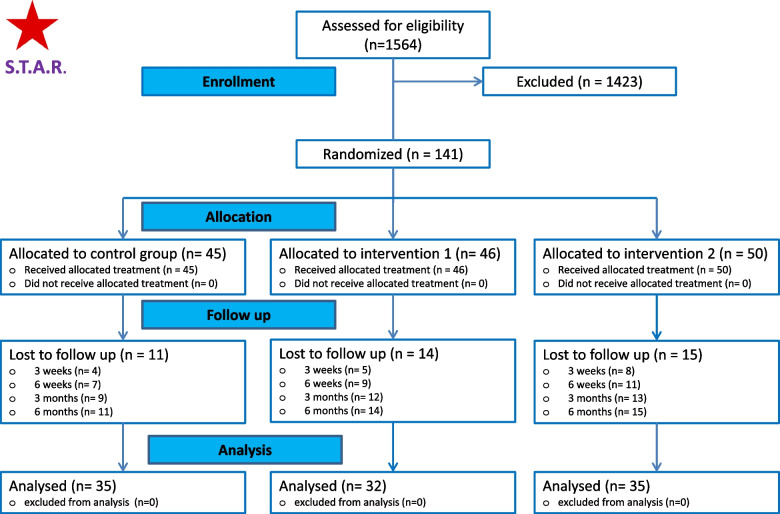
Methods: Participants were randomized to one of three study arms: Usual Care (UC), that is oral pain medication with or without physiotherapy, n = 45); intervention group 1: UC and transforaminal epidural steroid injection (TESI) 1 ml of 0.5% Levobupivacaine and 1 ml of 40 mg/ml Methylprednisolone and intervention group 2: UC and transforaminal epidural injection (TEI) with 1 ml of 0,5% Levobupivacaine and 1 ml of 0.9% NaCl (n = 50). The primary effect measure was health-related quality of life. Secondary outcomes were pain, functioning, and recovery. Costs were measured from a societal perspective, meaning that all costs were included, irrespective of who paid or benefited. Missing data were imputed using multiple imputation, and bootstrapping was used to estimate statistical uncertainty.
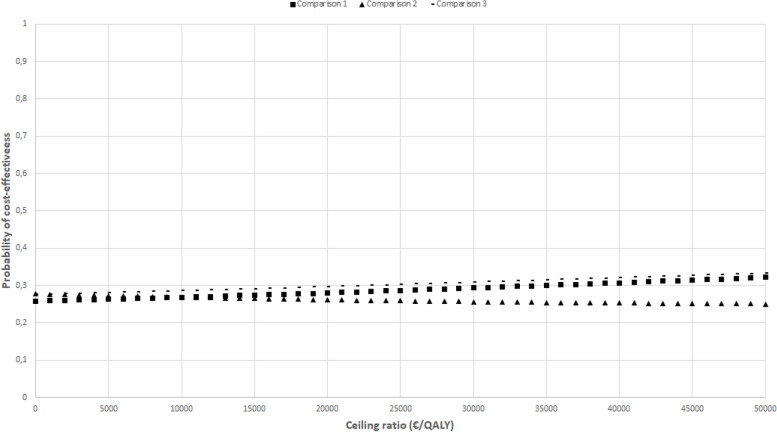
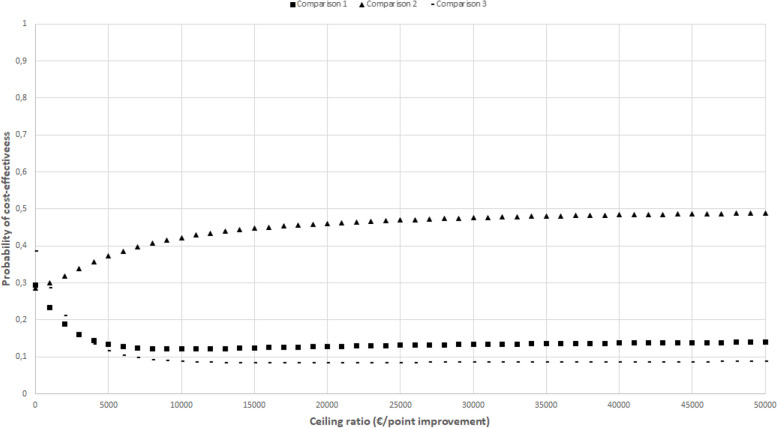
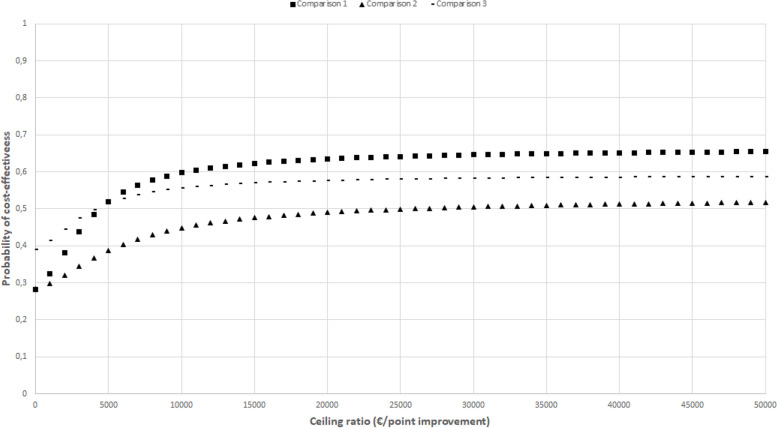
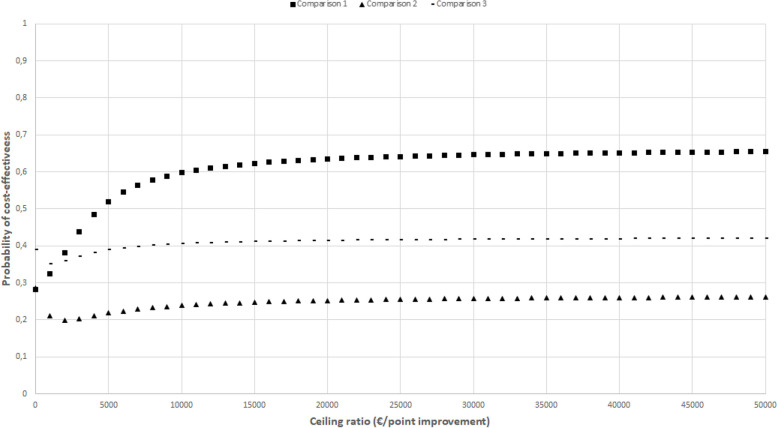
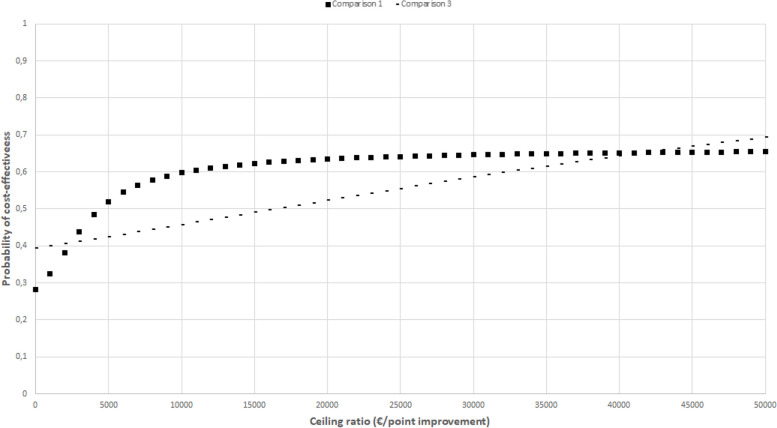
Results: None of the between-group differences in effects were statistically significant for any of the outcomes (QALY, back pain, leg pain, functioning, and global perceived effect) at the 26-weeks follow-up. The adjusted mean difference in total societal costs was €1718 (95% confidence interval [CI]: - 3020 to 6052) for comparison 1 (intervention group 1 versus usual care), €1640 (95%CI: - 3354 to 6106) for comparison 2 (intervention group 1 versus intervention group 2), and €770 (95%CI: - 3758 to 5702) for comparison 3 (intervention group 2 versus usual care). Except for the intervention costs, none of the aggregate and disaggregate cost differences were statistically significant. The maximum probability of all interventions being cost-effective compared to the control was low (< 0.7) for all effect measures.
Conclusion: These results suggest that adding TESI (or TEI) to usual care is not cost-effective compared to usual care in patients with acute sciatica (< 8 weeks) from a societal perspective in a Dutch healthcare setting.
Trial registration: Dutch National trial register: NTR4457 (March, 6th, 2014).
Keywords: Economic evaluation; Lumbar disc herniation; Randomized controlled trial; Sciatica; Transforaminal epidural steroid injections.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ropper AH, Zafonte RD. Sciatica. N Engl J Med 2015 26;372(13):1240–8. - PubMed
-
- El Barzouhi A, Verwoerd AJ, Peul WC, Verhagen AP, Lycklama À Nijeholt GJ, Van der Kallen BF, Koes BW, Vleggeert-Lankamp CL; Leiden–The Hague Spine Intervention Prognostic Study Group. Prognostic value of magnetic resonance imaging findings in patients with sciatica. J Neurosurg Spine. 2016;24(6):978–85. - PubMed
-
- Spijker-Huiges A, Groenhof F, Winters JC, van Wijhe M, Groenier KH, van der Meer K. Radiating low back pain in general practice: incidence, prevalence, diagnosis, and long-term clinical course of illness. Scand J Prim Health Care. 2015;33(1):27–32. doi: 10.3109/02813432.2015.1006462. - DOI - PMC - PubMed
-
- Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine (Phila Pa 1976). 2008;33(22):2464–72. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
