

Enhanced recovery after liver surgery in cirrhotic patients: a systematic review and meta-analysis
- PMID: 38561792
- PMCID: PMC10983761
- DOI: 10.1186/s13741-024-00375-x
Enhanced recovery after liver surgery in cirrhotic patients: a systematic review and meta-analysis
Abstract
Background: Few studies have assessed enhanced recovery after surgery (ERAS) in liver surgery for cirrhotic patients. The present meta-analysis assessed the impact of ERAS pathways on outcomes after liver surgery in cirrhotic patients compared to standard care.
Methods: A literature search was performed on PubMed/MEDLINE, Embase, and the Cochrane Library. Studies comparing ERAS protocols versus standard care in cirrhotic patients undergoing liver surgery were included. The primary outcome was post-operative complications, while secondary outcomes were mortality rates, length of stay (LoS), readmissions, reoperations, and liver failure rates.
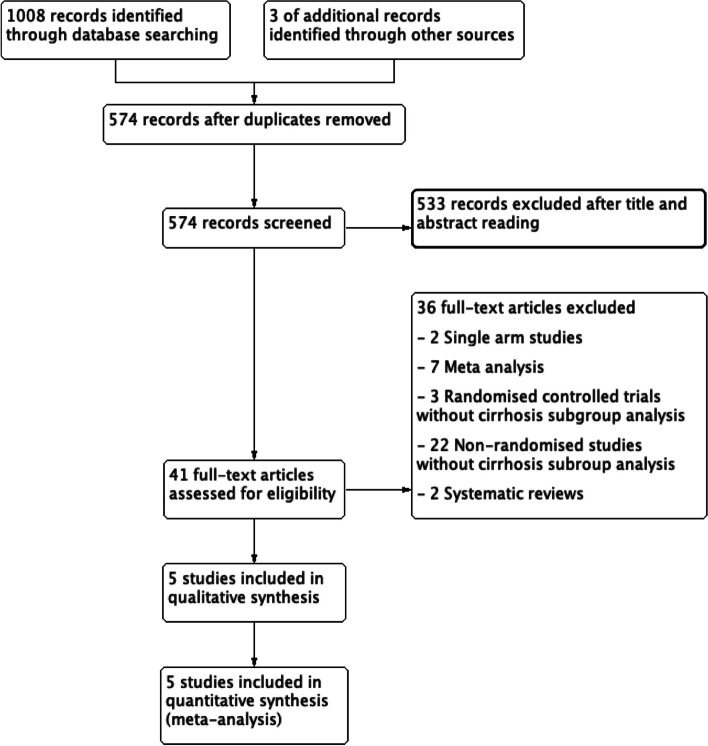
Results: After evaluating 41 full-text manuscripts, 5 articles totaling 646 patients were included (327 patients in the ERAS group and 319 in the non-ERAS group). Compared to non-ERAS care, ERAS patients had less risk of developing overall complications (OR 0.43, 95% CI 0.31-0.61, p < 0.001). Hospitalization was on average 2 days shorter for the ERAS group (mean difference - 2.04, 95% CI - 3.19 to - 0.89, p < 0.001). Finally, no difference was found between both groups concerning 90-day post-operative mortality and rates of reoperations, readmissions, and liver failure.
Conclusion: In cirrhotic patients, ERAS protocol for liver surgery is safe and decreases post-operative complications and LoS. More randomized controlled trials are needed to confirm the results of the present analysis.
Keywords: ERAS; Fibrosis; Hepatectomy; Hepatic resection; Perioperative care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




Similar articles
-
Enhanced recovery after surgery programs in patients undergoing hepatectomy: A meta-analysis.World J Gastroenterol. 2015 Aug 14;21(30):9209-16. doi: 10.3748/wjg.v21.i30.9209. World J Gastroenterol. 2015. PMID: 26290648 Free PMC article. Review.
-
Enhanced Recovery After Surgery (ERAS) protocols following emergency intra-abdominal surgery: A systematic review and meta-analysis protocol.PLoS One. 2023 Sep 8;18(9):e0291140. doi: 10.1371/journal.pone.0291140. eCollection 2023. PLoS One. 2023. PMID: 37682876 Free PMC article.
-
Systematic review and meta-analysis of the clinical utility of Enhanced Recovery After Surgery pathways in adult spine surgery.J Neurosurg Spine. 2020 Nov 6;34(2):325-347. doi: 10.3171/2020.6.SPINE20795. Print 2021 Feb 1. J Neurosurg Spine. 2020. PMID: 33157522
-
Enhanced recovery after surgery (ERAS) versus standard recovery for elective gastric cancer surgery: A meta-analysis of randomized controlled trials.Surg Oncol. 2020 Mar;32:75-87. doi: 10.1016/j.suronc.2019.11.004. Epub 2019 Nov 25. Surg Oncol. 2020. PMID: 31786352
-
Enhanced recovery care versus traditional care after laparoscopic liver resections: a randomized controlled trial.Surg Endosc. 2018 Jun;32(6):2746-2757. doi: 10.1007/s00464-017-5973-3. Epub 2017 Dec 12. Surg Endosc. 2018. PMID: 29234943 Clinical Trial.
Cited by
-
Specific Items of Enhanced Recovery After Surgery for Liver Surgery in Cirrhotic Patients: A Systematic Review.World J Surg. 2025 Aug;49(8):2125-2143. doi: 10.1002/wjs.12677. Epub 2025 Jun 23. World J Surg. 2025. PMID: 40551534 Free PMC article. Review.
References
-
- Bell R, Ward D, Jeffery J, Toogood GJ, Lodge JpA, Rao K, et al. A randomized controlled trial comparing epidural analgesia versus continuous local anesthetic infiltration via abdominal wound catheter in open liver resection. Ann Surg. 2019;269(3):413–9. doi: 10.1097/SLA.0000000000002988. - DOI - PubMed
-
- Benzoni E, Molaro R, Cedolini C, Favero A, Cojutti A, Lorenzin D, et al. Liver resection for HCC: analysis of causes and risk factors linked to postoperative complications. Hepatogastroenterology. 2007;54(73):186–9. - PubMed
LinkOut - more resources
Full Text Sources
