

"NeuroVanguard": a contemporary strategy in neuromonitoring for severe adult brain injury patients
- PMID: 38561829
- PMCID: PMC10985991
- DOI: 10.1186/s13054-024-04893-4
"NeuroVanguard": a contemporary strategy in neuromonitoring for severe adult brain injury patients
Abstract
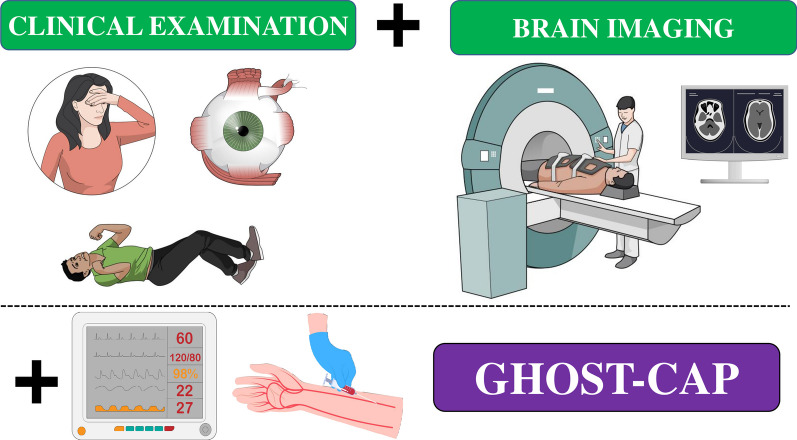
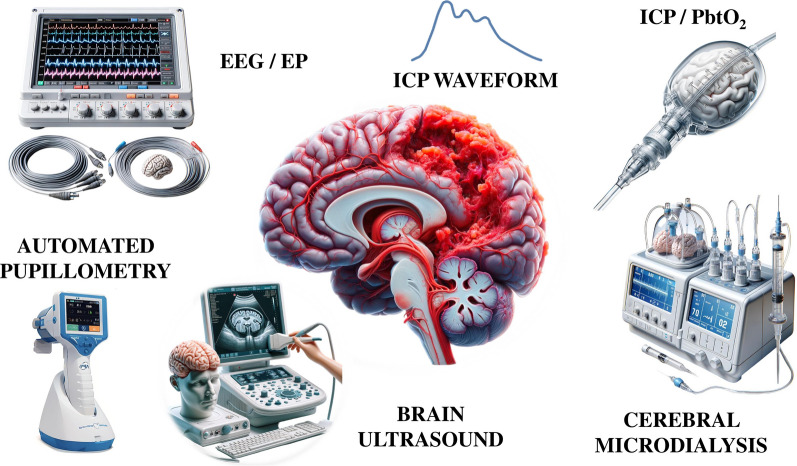
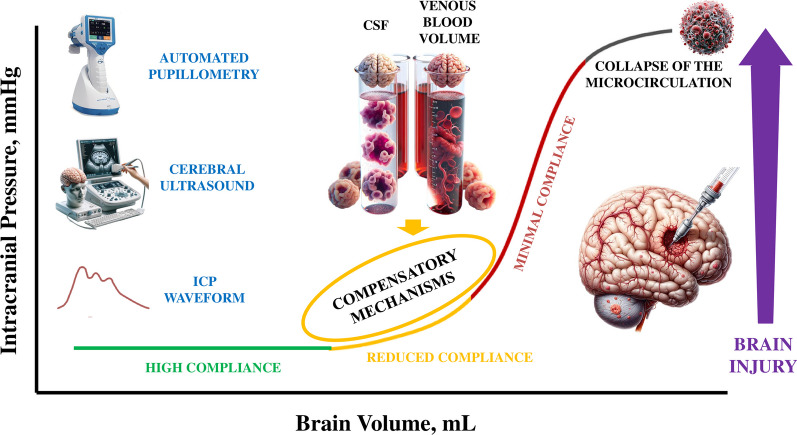
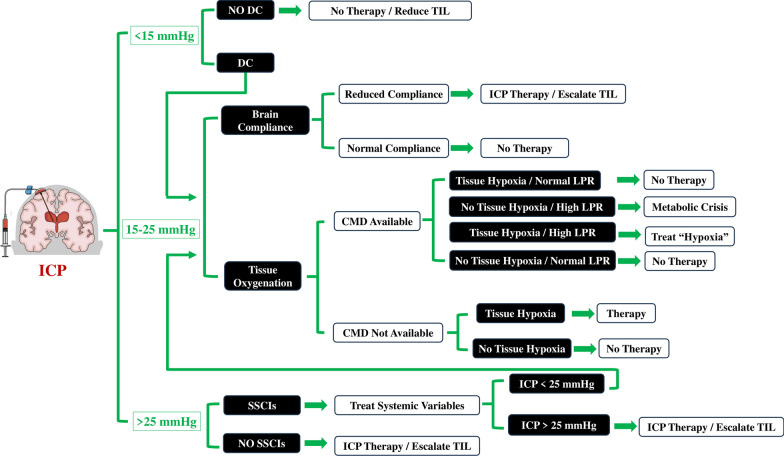
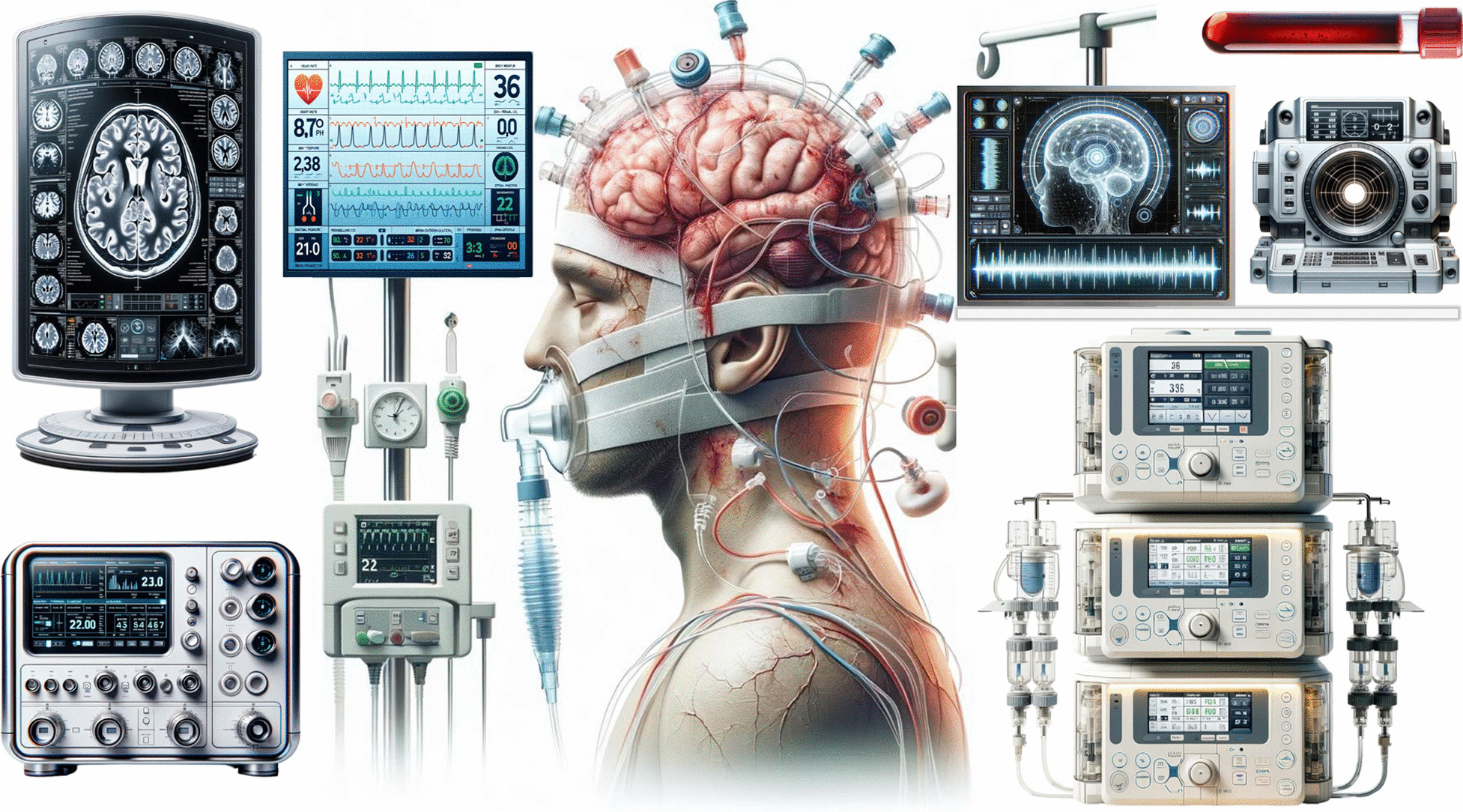
Severe acute brain injuries, stemming from trauma, ischemia or hemorrhage, remain a significant global healthcare concern due to their association with high morbidity and mortality rates. Accurate assessment of secondary brain injuries severity is pivotal for tailor adequate therapies in such patients. Together with neurological examination and brain imaging, monitoring of systemic secondary brain injuries is relatively straightforward and should be implemented in all patients, according to local resources. Cerebral secondary injuries involve factors like brain compliance loss, tissue hypoxia, seizures, metabolic disturbances and neuroinflammation. In this viewpoint, we have considered the combination of specific noninvasive and invasive monitoring tools to better understand the mechanisms behind the occurrence of these events and enhance treatment customization, such as intracranial pressure monitoring, brain oxygenation assessment and metabolic monitoring. These tools enable precise intervention, contributing to improved care quality for severe brain injury patients. The future entails more sophisticated technologies, necessitating knowledge, interdisciplinary collaboration and resource allocation, with a focus on patient-centered care and rigorous validation through clinical trials.
Keywords: Acute brain injury; Individualized care; Integrated physiology; Neuromonitoring.
© 2024. The Author(s).
Conflict of interest statement
FST received lecture fees from Integra Lifesciences and is Scientific Advisor for Neuroptics and Nihon Khoden. Other authors have no competing interests to declare.
Figures
Comment in
-
Adapting NeuroVanguard to real-world challenges.Crit Care. 2024 Apr 23;28(1):137. doi: 10.1186/s13054-024-04916-0. Crit Care. 2024. PMID: 38654362 Free PMC article. No abstract available.
-
The neurovanguard concept and real-world embracement.Crit Care. 2024 May 8;28(1):153. doi: 10.1186/s13054-024-04941-z. Crit Care. 2024. PMID: 38720380 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
