

Effect of Patellar Morphology on the Risk of Osteochondral Fracture after Patellar Dislocation: A Cross-sectional Study
- PMID: 38561949
- PMCID: PMC11062850
- DOI: 10.1111/os.14036
Effect of Patellar Morphology on the Risk of Osteochondral Fracture after Patellar Dislocation: A Cross-sectional Study
Abstract
Objective: The risk of osteochondral fracture (OCF) after patellar dislocation has been shown to be related to patellofemoral anatomy, but its relationship to patellar morphology remains unknown. The aim of this study was to investigate the associations between patellar morphology and the risk of OCF after patellar dislocation.
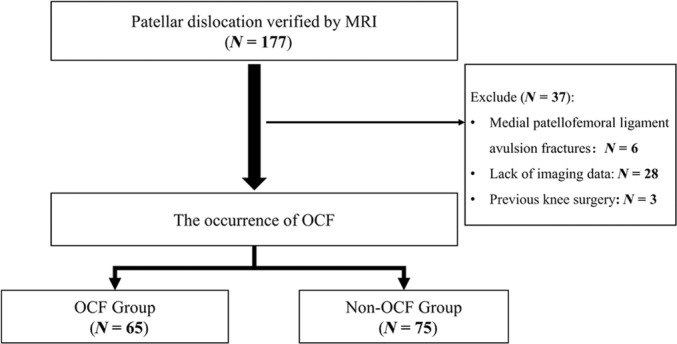
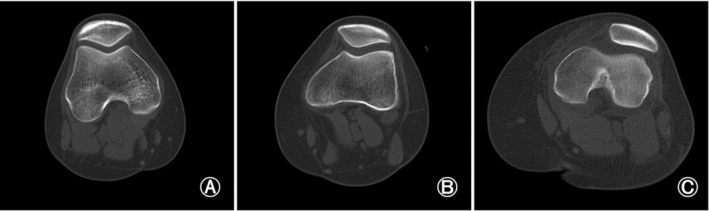
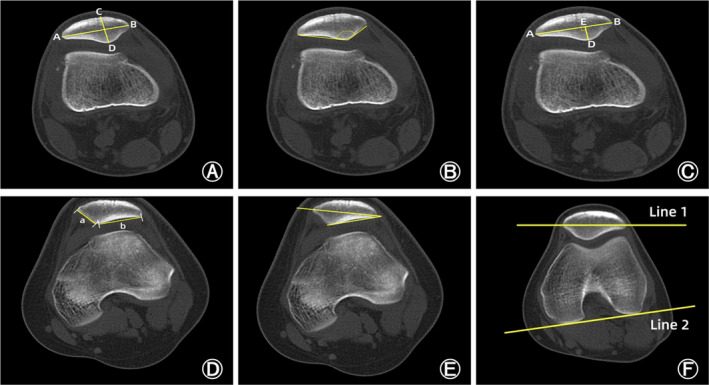
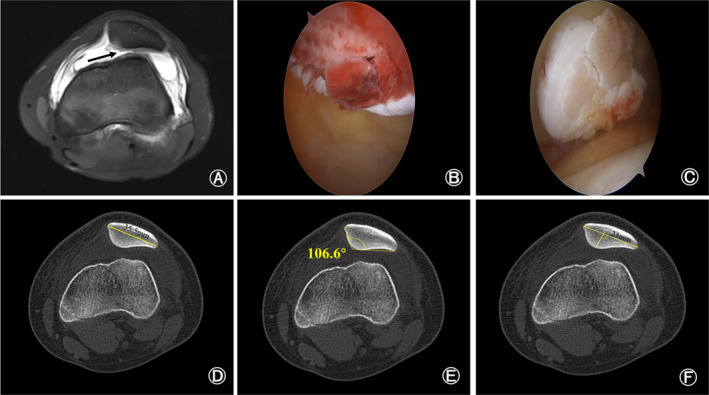
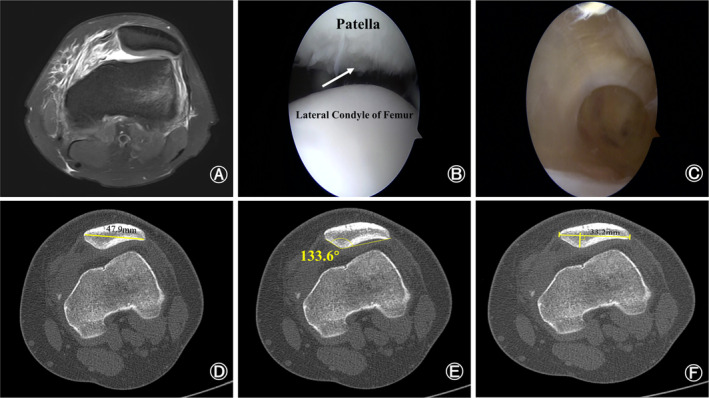
Methods: A total of 140 patients with patellar dislocation between January 2018 and June 2023 were enrolled in this study and divided into two groups. Sixty-five patellar dislocation patients with OCF were included in the OCF group, while 75 patellar dislocation patients without OCF were included in the non-OCF group. Computed tomography was used to compare measurements of patellar morphology including Wiberg classification, patellar width and thickness, Wiberg angle, Wiberg index, facet ratio, lateral patellar facet angle, and patellar tilt angle. A logistic regression model was performed to evaluate the correlations between patellar morphology and the risk of OCF after patellar dislocation. Receiver operating characteristic curves were used to calculate the area under the curve (AUC) and determine the diagnostic values of patellar morphology for OCF after patellar dislocation. Subgroup analyses for gender and age were conducted to compare the differences in patellar morphology of PD patients.
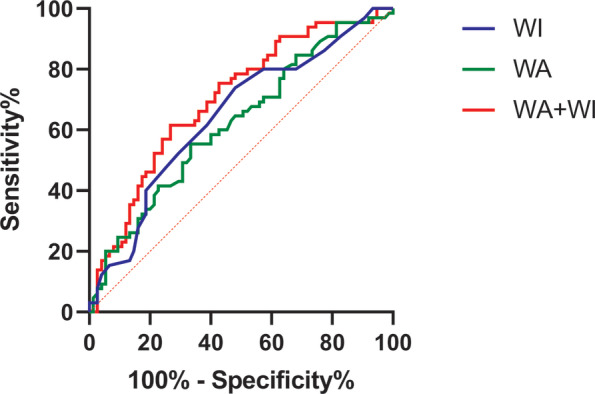
Results: Wiberg angle was significantly lower in the OCF group (p = 0.017), while Wiberg index (p = 0.002) and facet ratio (p = 0.023) were significantly higher in the OCF group. According to the results of logistic regression analysis, Wiberg angle (odds ratio [OR] = 0.96, p = 0.022) and Wiberg index (OR = 1.105, p = 0.032) were the final relevant factors for the occurrence of OCF after patellar dislocation. The AUC was 0.622 (95% confidence interval [CI]: 0.529-0.714) for Wiberg angle, 0.65 (95% CI: 0.558-0.742) for Wiberg index, and 0.702 (95% CI: 0.615-0.788) for the combination of Wiberg angle plus Wiberg index.
Conclusion: Wiberg angle and Wiberg index were independent risk factors for the occurrence of osteochondral fracture after patellar dislocation. Moreover, Wiberg angle, Wiberg index, and the combination of Wiberg angle plus Wiberg index had good predictive diagnostic value for the occurrence of OCF after patellar dislocation.
Keywords: Computed tomography; Osteochondral fracture; Patellar dislocation; Patellar morphology; Patellofemoral instability.
© 2024 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Sulcus depth, congruence angle, Wiberg index, TT-TG distance, and CDI are strong predictors of recurrent patellar dislocation.Knee Surg Sports Traumatol Arthrosc. 2023 Jul;31(7):2906-2916. doi: 10.1007/s00167-022-07245-3. Epub 2022 Dec 4. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36463567
-
The risk of osteochondral fracture after patellar dislocation is related to patellofemoral anatomy.Knee Surg Sports Traumatol Arthrosc. 2021 Dec;29(12):4241-4250. doi: 10.1007/s00167-021-06547-2. Epub 2021 Mar 28. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 33774692
-
Anatomic Risk Factors for Osteochondral Fracture of Acute First-Time Patellar Dislocation in Adolescents: A Retrospective Magnetic Resonance Imaging Study.Evid Based Complement Alternat Med. 2022 Aug 8;2022:6723326. doi: 10.1155/2022/6723326. eCollection 2022. Evid Based Complement Alternat Med. 2022. Retraction in: Evid Based Complement Alternat Med. 2023 Jul 19;2023:9786026. doi: 10.1155/2023/9786026. PMID: 35979012 Free PMC article. Retracted.
-
Assessment of Patellar Morphology in Trochlear Dysplasia on Computed Tomography Scans.Orthop Surg. 2021 Apr;13(2):458-465. doi: 10.1111/os.12825. Epub 2021 Jan 24. Orthop Surg. 2021. PMID: 33491266 Free PMC article.
-
Treatment of Osteochondral Fractures After Acute Patellofemoral Instability: A Critical Analysis Review.JBJS Rev. 2022 Apr 8;10(4). doi: 10.2106/JBJS.RVW.21.00242. JBJS Rev. 2022. PMID: 35394969 Review.
References
-
- Fithian DC, Paxton EW, Stone ML, Silva P, Davis DK, Elias DA, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med. 2004;32(5):1114–1121. - PubMed
-
- Christensen TC, Sanders TL, Pareek A, Mohan R, Dahm DL, Krych AJ. Risk factors and time to recurrent ipsilateral and contralateral patellar dislocations. Am J Sports Med. 2017;45(9):2105–2110. - PubMed
-
- Hiemstra LA, Kerslake S, Lafave M. Assessment of demographic and pathoanatomic risk factors in recurrent patellofemoral instability. Knee Surg Sports Traumatol Arthrosc. 2017;25(12):3849–3855. - PubMed
-
- Fox AJ, Wanivenhaus F, Rodeo SA. The basic science of the patella: structure, composition, and function. J Knee Surg. 2012;25(2):127–141. - PubMed
