

This is a preprint.
A potential neuromodulation target for PTSD in Veterans derived from focal brain lesions
- PMID: 38562753
- PMCID: PMC10984085
- DOI: 10.21203/rs.3.rs-3132332/v1
A potential neuromodulation target for PTSD in Veterans derived from focal brain lesions
Update in
-
A potential target for noninvasive neuromodulation of PTSD symptoms derived from focal brain lesions in veterans.Nat Neurosci. 2024 Nov;27(11):2231-2239. doi: 10.1038/s41593-024-01772-7. Epub 2024 Sep 24. Nat Neurosci. 2024. PMID: 39317797
Abstract
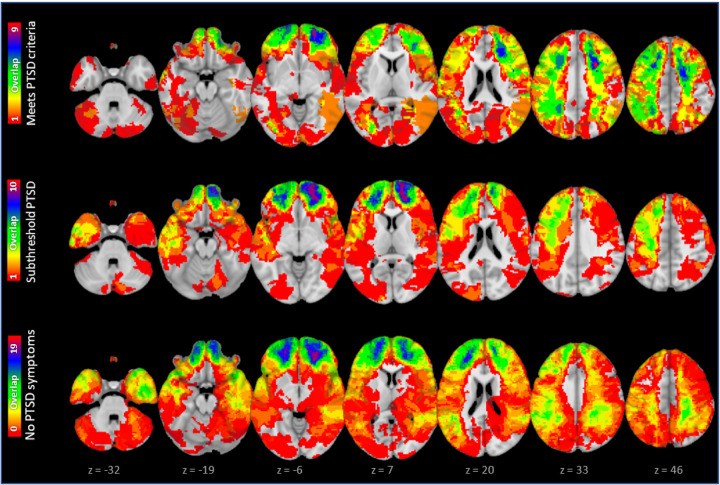
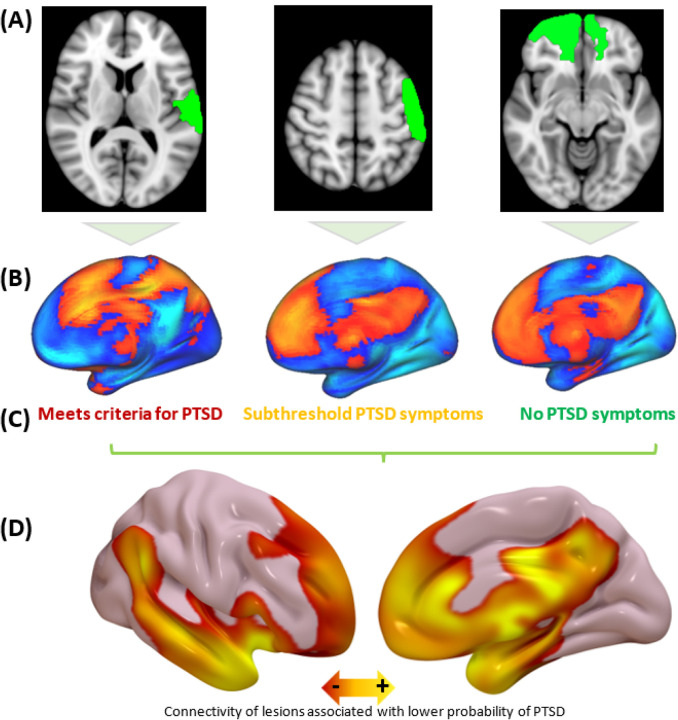
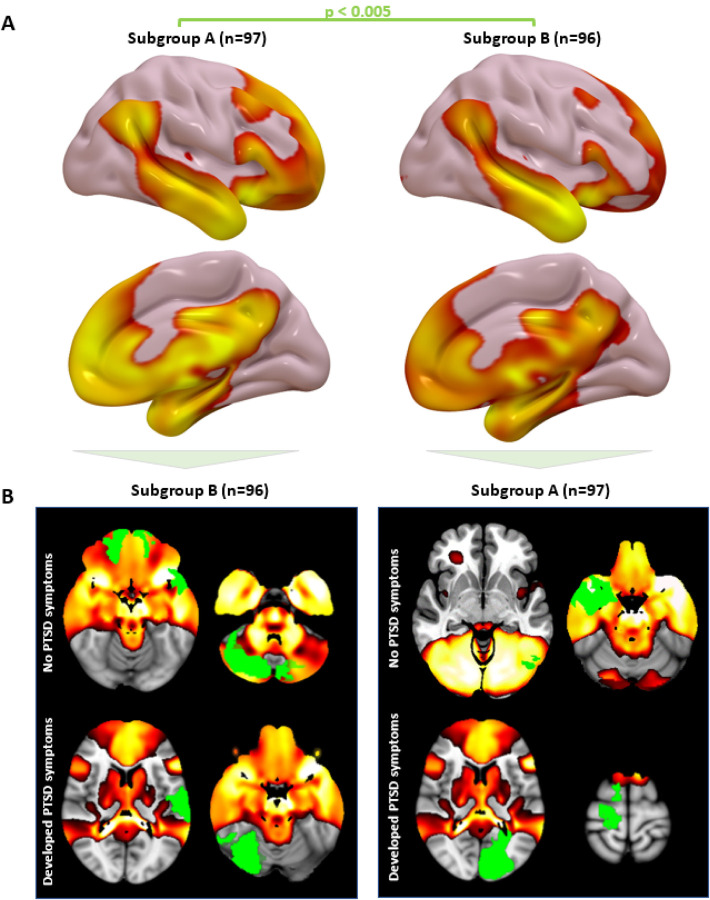
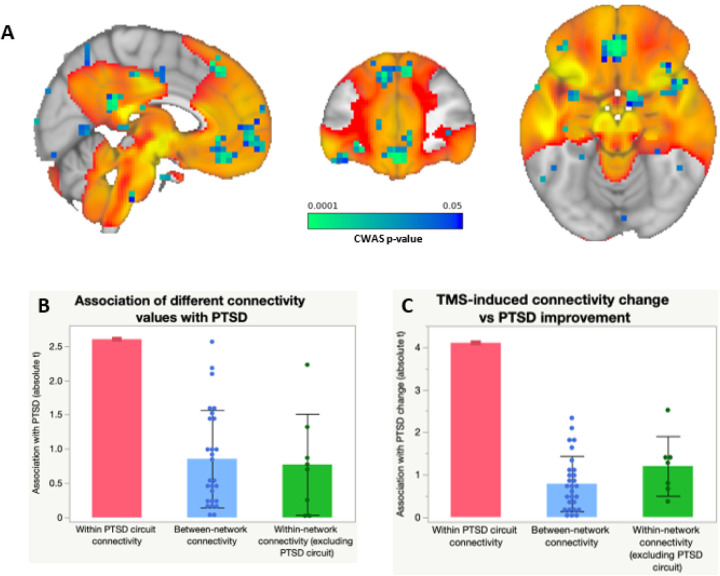
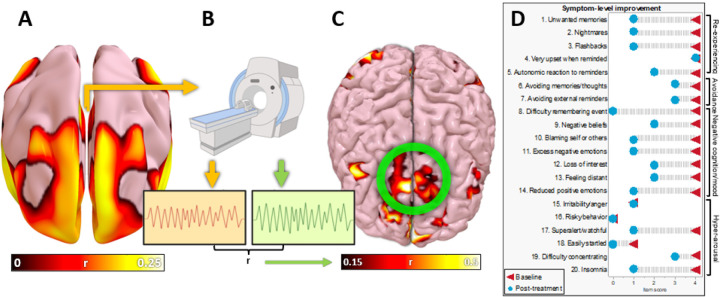
Neuromodulation trials for PTSD have yielded mixed results, and the optimal neuroanatomical target remains unclear. We analyzed three datasets to study brain circuitry causally linked to PTSD in military Veterans. After penetrating traumatic brain injury (n=193), lesions that reduced probability of PTSD were preferentially connected to a circuit including the medial prefrontal cortex (mPFC), amygdala, and anterolateral temporal lobe (cross-validation p=0.01). In Veterans without lesions (n=180), PTSD was specifically associated with connectivity within this circuit (p<0.01). Connectivity change within this circuit correlated with PTSD improvement after transcranial magnetic stimulation (TMS) (n=20) (p<0.01), even though the circuit was not directly targeted. Finally, we directly targeted this circuit with fMRI-guided accelerated TMS, leading to rapid resolution of symptoms in a patient with severe lifelong PTSD. All results were independent of depression severity. This lesion-based PTSD circuit may serve as a neuromodulation target for Veterans with PTSD.
Conflict of interest statement
SHS: Owner of intellectual property involving the use of brain connectivity to target TMS, scientific consultant for Magnus Medical, investigator-initiated research funding from Neuronetics and Brainsway, speaking fees from Brainsway and Otsuka (for PsychU.org), shareholder in Brainsway (publicly traded) and Magnus Medical (not publicly traded). None of these entities were directly involved in the present work. MDF: Scientific consultant for Magnus Medical, owns independent intellectual property involving the use of functional connectivity to target TMS. This intellectual property was not used in the present manuscript. NSP: Received clinical trial support (through VA contracts) from Wave Neuroscience and Neurolief, and serves on the scientific advisory board for Pulvinar Neuro.
Figures

Similar articles
-
A potential target for noninvasive neuromodulation of PTSD symptoms derived from focal brain lesions in veterans.Nat Neurosci. 2024 Nov;27(11):2231-2239. doi: 10.1038/s41593-024-01772-7. Epub 2024 Sep 24. Nat Neurosci. 2024. PMID: 39317797
-
Repetitive Transcranial Magnetic Stimulation for Depression and Posttraumatic Stress Disorder in Veterans With Mild Traumatic Brain Injury.Neuromodulation. 2023 Jun;26(4):878-884. doi: 10.1016/j.neurom.2022.11.015. Epub 2023 Feb 1. Neuromodulation. 2023. PMID: 36737300 Free PMC article.
-
Prefrontal transcranial magnetic stimulation for depression in US military veterans - A naturalistic cohort study in the veterans health administration.J Affect Disord. 2022 Jan 15;297:671-678. doi: 10.1016/j.jad.2021.10.025. Epub 2021 Oct 20. J Affect Disord. 2022. PMID: 34687780 Free PMC article.
-
Deep Brain Stimulation for Post-Traumatic Stress Disorder: A Review of the Experimental and Clinical Literature.Stereotact Funct Neurosurg. 2022;100(3):143-155. doi: 10.1159/000521130. Epub 2022 Jan 3. Stereotact Funct Neurosurg. 2022. PMID: 34979516 Review.
-
Application of Deep Brain Stimulation in Refractory Post-Traumatic Stress Disorder.Cureus. 2023 Jan 14;15(1):e33780. doi: 10.7759/cureus.33780. eCollection 2023 Jan. Cureus. 2023. PMID: 36819333 Free PMC article. Review.
References
Publication types
Grants and funding
- I21 RX002032/RX/RRD VA/United States
- I01 CX002293/CX/CSRD VA/United States
- I50 RX002864/RX/RRD VA/United States
- R01 NS086885/NS/NINDS NIH HHS/United States
- R01 AG060987/AG/NIA NIH HHS/United States
- P20 GM130452/GM/NIGMS NIH HHS/United States
- U01 MH123427/MH/NIMH NIH HHS/United States
- R21 MH126271/MH/NIMH NIH HHS/United States
- K23 MH121657/MH/NIMH NIH HHS/United States
- R56 AG069086/AG/NIA NIH HHS/United States
- R01 MH115949/MH/NIMH NIH HHS/United States
- R01 MH113929/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
