

This is a preprint.
Unsupervised machine learning analysis to identify patterns of ICU medication use for fluid overload prediction
- PMID: 38562806
- PMCID: PMC10984037
- DOI: 10.1101/2024.03.21.24304663
Unsupervised machine learning analysis to identify patterns of ICU medication use for fluid overload prediction
Update in
-
Unsupervised machine learning analysis to identify patterns of ICU medication use for fluid overload prediction.Pharmacotherapy. 2025 Feb;45(2):76-86. doi: 10.1002/phar.4642. Epub 2025 Jan 3. Pharmacotherapy. 2025. PMID: 39749877
Abstract
Introduction: Intravenous (IV) medications are a fundamental cause of fluid overload (FO) in the intensive care unit (ICU); however, the association between IV medication use (including volume), administration timing, and FO occurrence remains unclear.
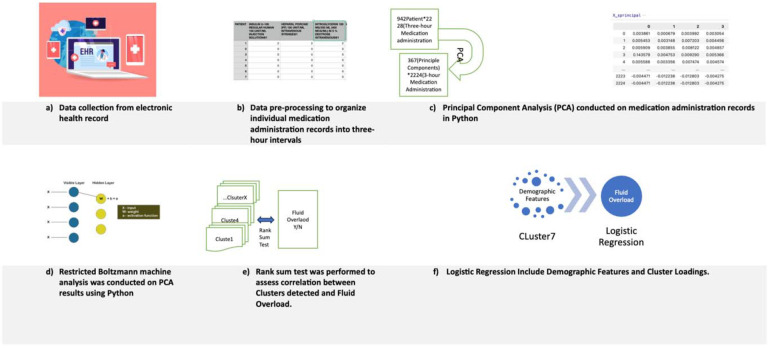
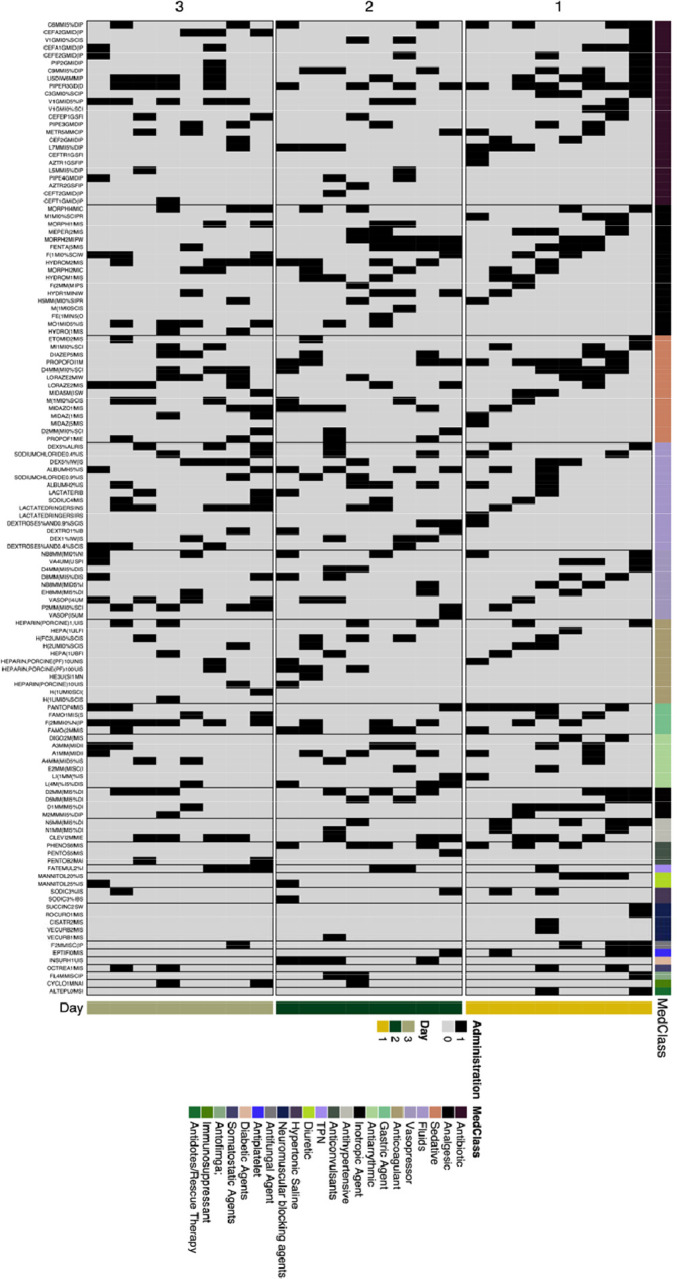
Methods: This retrospective cohort study included consecutive adults admitted to an ICU ≥72 hours with available fluid balance data. FO was defined as a positive fluid balance ≥7% of admission body weight within 72 hours of ICU admission. After reviewing medication administration record (MAR) data in three-hour periods, IV medication exposure was categorized into clusters using principal component analysis (PCA) and Restricted Boltzmann Machine (RBM). Medication regimens of patients with and without FO were compared within clusters to assess for temporal clusters associated with FO using the Wilcoxon rank sum test. Exploratory analyses of the medication cluster most associated with FO for medications frequently appearing and used in the first 24 hours was conducted.
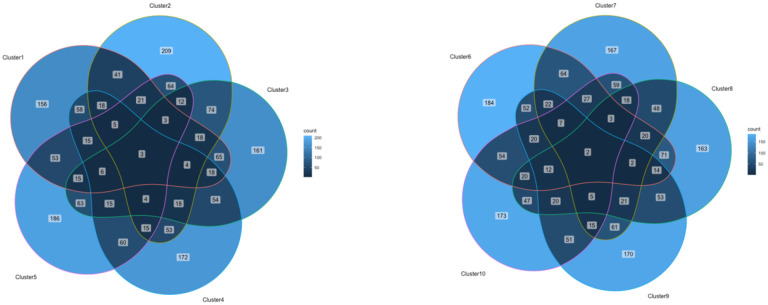
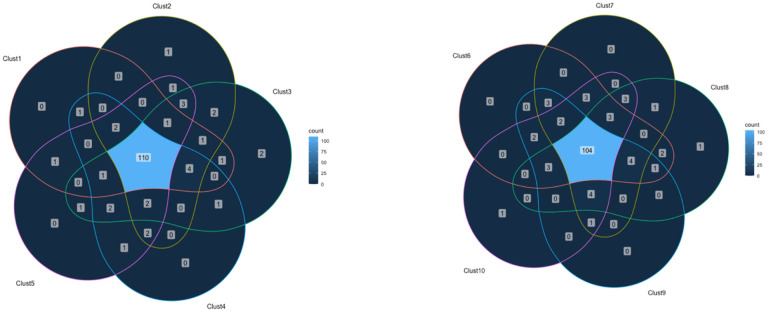
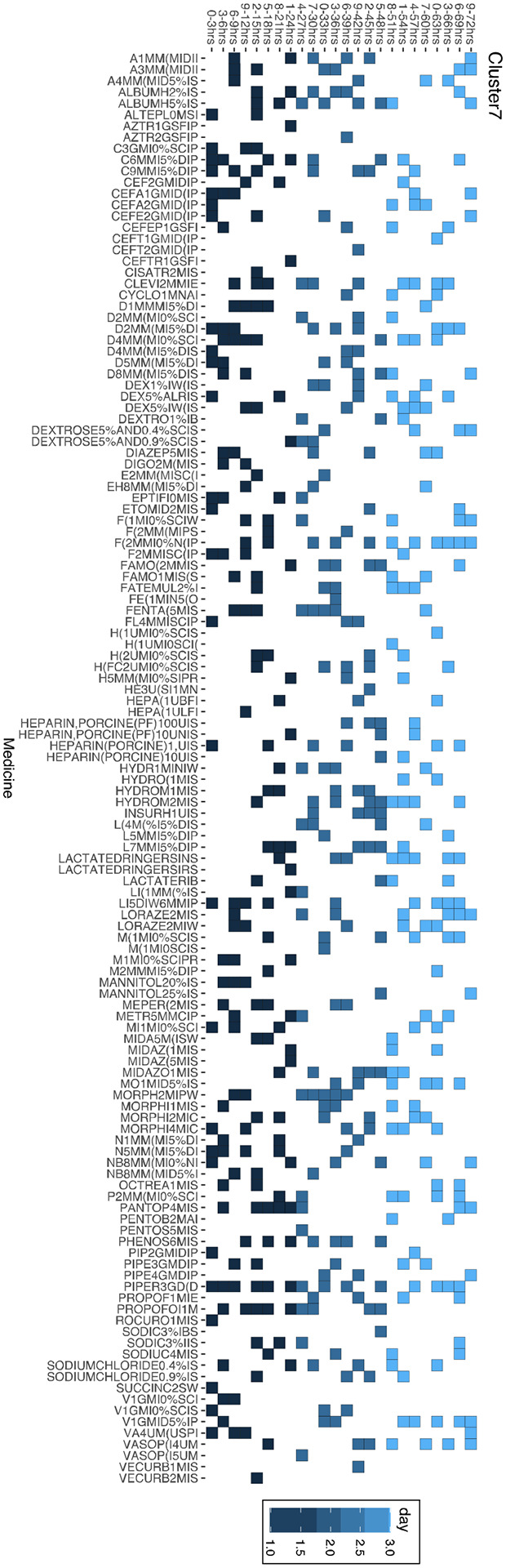
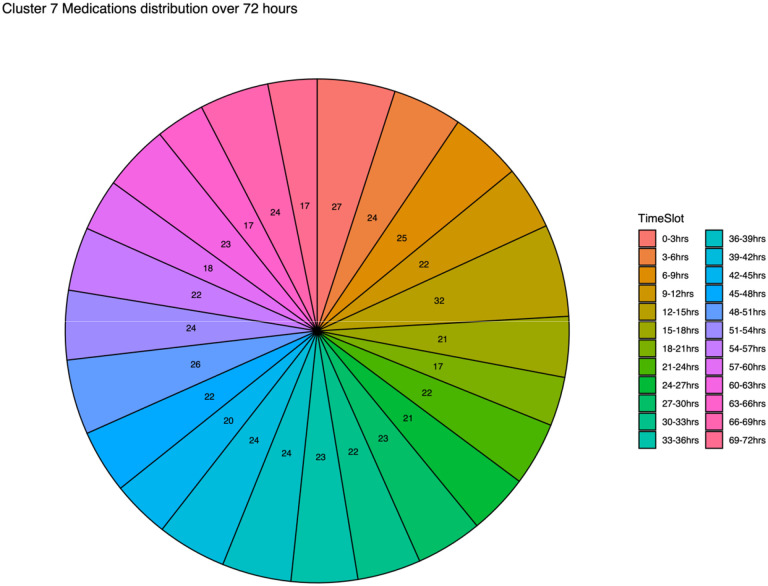
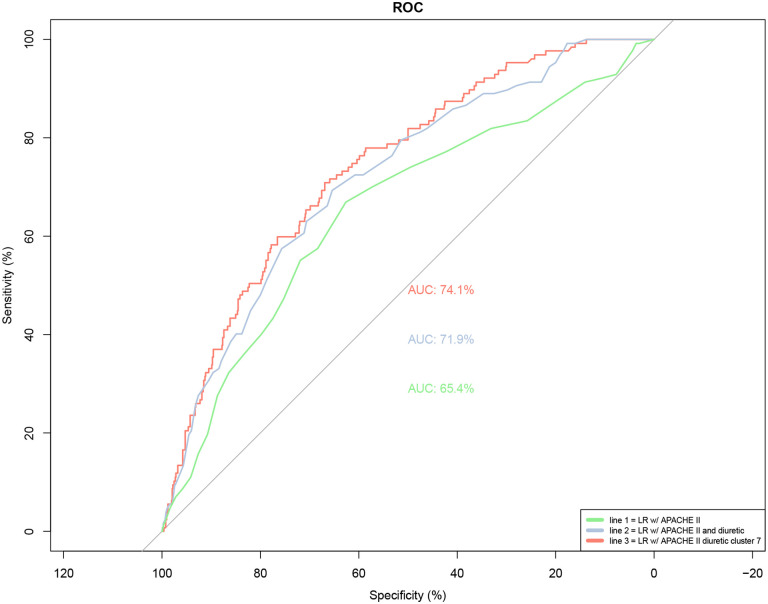
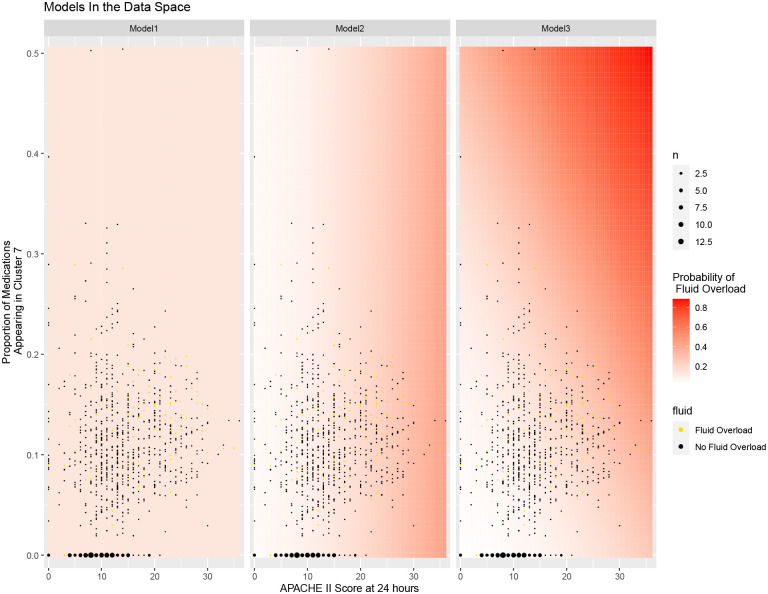
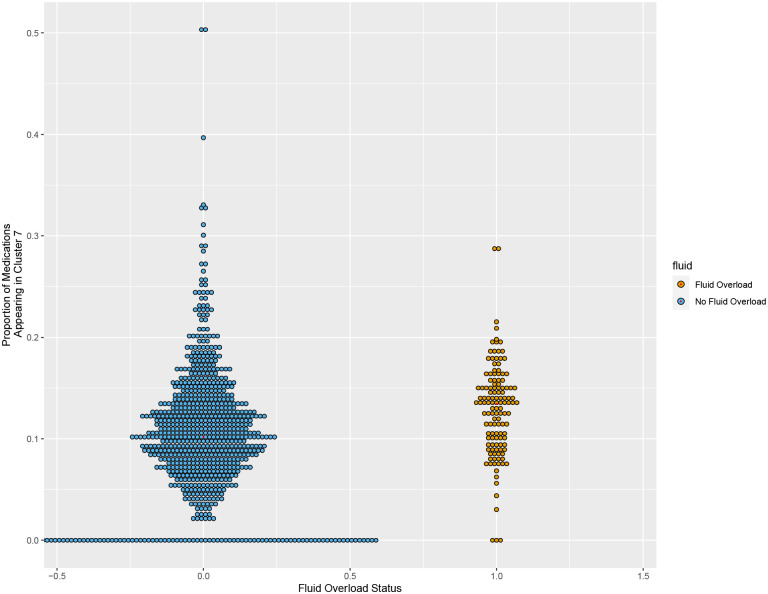
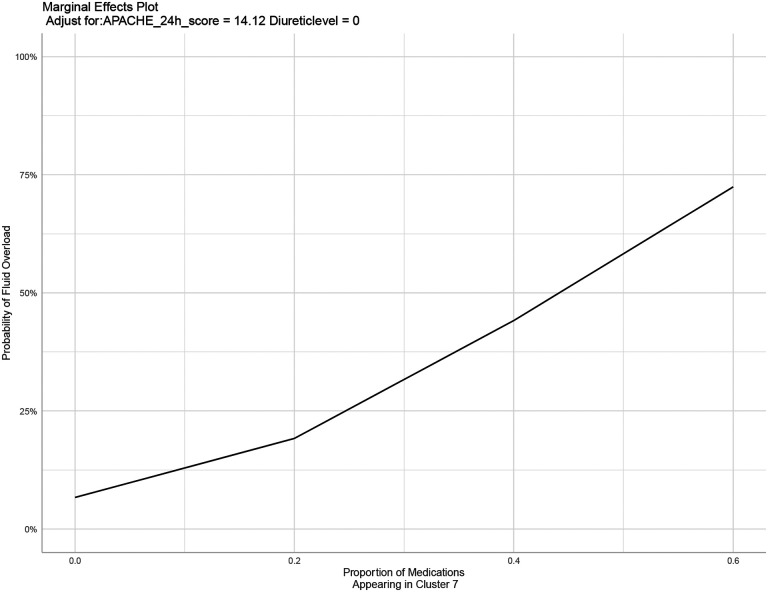
Results: FO occurred in 127/927 (13.7%) of the patients enrolled. Patients received a median (IQR) of 31 (13-65) discrete IV medication administrations over the 72-hour period. Across all 47,803 IV medication administrations, ten unique IV medication clusters were identified with 121-130 medications in each cluster. Among the ten clusters, cluster 7 had the greatest association with FO; the mean number of cluster 7 medications received was significantly greater in patients in the FO cohort compared to patients who did not experience FO (25.6 vs.10.9. p<0.0001). 51 of the 127 medications in cluster 7 (40.2%) appeared in > 5 separate 3-hour periods during the 72-hour study window. The most common cluster 7 medications included continuous infusions, antibiotics, and sedatives/analgesics. Addition of cluster 7 medications to a prediction model with APACHE II score and receipt of diuretics improved the ability for the model to predict fluid overload (AUROC 5.65, p =0.0004).
Conclusions: Using ML approaches, a unique IV medication cluster was strongly associated with FO. Incorporation of this cluster improved the ability to predict development of fluid overload in ICU patients compared with traditional prediction models. This method may be further developed into real-time clinical applications to improve early detection of adverse outcomes.
Keywords: critical care; fluid overload; machine learning; medication regimen complexity; prediction.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest.
Figures

Similar articles
-
Unsupervised machine learning analysis to identify patterns of ICU medication use for fluid overload prediction.Pharmacotherapy. 2025 Feb;45(2):76-86. doi: 10.1002/phar.4642. Epub 2025 Jan 3. Pharmacotherapy. 2025. PMID: 39749877
-
Pharmacophenotype identification of intensive care unit medications using unsupervised cluster analysis of the ICURx common data model.Crit Care. 2023 May 2;27(1):167. doi: 10.1186/s13054-023-04437-2. Crit Care. 2023. PMID: 37131200 Free PMC article.
-
Machine learning vs. traditional regression analysis for fluid overload prediction in the ICU.Sci Rep. 2023 Nov 10;13(1):19654. doi: 10.1038/s41598-023-46735-3. Sci Rep. 2023. PMID: 37949982 Free PMC article.
-
Fluid Overload in Critically Ill Children.Front Pediatr. 2018 Oct 29;6:306. doi: 10.3389/fped.2018.00306. eCollection 2018. Front Pediatr. 2018. PMID: 30420946 Free PMC article. Review.
-
Association between fluid overload and mortality in children with sepsis: a systematic review and meta-analysis.BMJ Paediatr Open. 2023 Nov;7(1):e002094. doi: 10.1136/bmjpo-2023-002094. BMJ Paediatr Open. 2023. PMID: 37989355 Free PMC article.
References
-
- Hawkins WA, Butler SA, Poirier N, et al.: From theory to bedside: implementation of fluid stewardship in a medical ICU pharmacy practice. Am J Health Syst Pharm 2022. Jun 7;79(12):984–992. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources