

Characteristics and Prognosis of Type 2 Myocardial Infarction Through Worsening Renal Function and NT-proBNP in Older Adults with Pneumonia
- PMID: 38562970
- PMCID: PMC10984204
- DOI: 10.2147/CIA.S438541
Characteristics and Prognosis of Type 2 Myocardial Infarction Through Worsening Renal Function and NT-proBNP in Older Adults with Pneumonia
Abstract
Background: Type 2 myocardial infarction (MI) is becoming more recognized. This study aimed to assess the factors linked to type 2 MI in older adults with pneumonia and further determine the predictive factors of 90-day adverse events (refractory heart failure, cardiogenic shock, and all-cause mortality).
Methods: A single-center retrospective analysis was conducted among older adults with pneumonia. The primary outcome was the prevalence of type 2 MI. The secondary objective was to assess the adverse events in these patients with type 2 MI within 90 days.
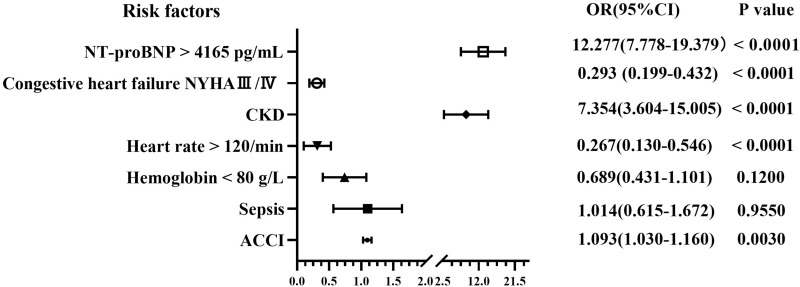
Results: A total of 2618 patients were included. Of these, 361 patients (13.8%) suffered from type 2 MI. Multivariable predictors of type 2 MI were chronic kidney disease (CKD), age-adjusted Charlson comorbidity index (ACCI) score, and NT-proBNP > 4165pg/mL. Moreover, the independent predictive factors of 90-day adverse events included NT-proBNP > 4165pg/mL, age, ACCI score, and CKD. The Kaplan-Meier adverse events curves revealed that the type 2 MI patients with CKD and NT-proBNP > 4165pg/mL had a higher risk than CKD or NT-proBNP > 4165pg/mL alone.
Conclusion: Type 2 MI in older pneumonia hospitalization represents a heterogeneous population. Elevated NT-proBNP level and prevalence of CKD are important predictors of type 2 MI and 90-day adverse events in type 2 MI patients.
Keywords: mortality; older; pneumonia; type 2 myocardial infarction.
© 2024 Ma et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
