

Long-Term Clinical-Pathologic Results of Enzyme Replacement Therapy in Prehypertrophic Fabry Disease Cardiomyopathy
- PMID: 38563373
- PMCID: PMC11262509
- DOI: 10.1161/JAHA.123.032734
Long-Term Clinical-Pathologic Results of Enzyme Replacement Therapy in Prehypertrophic Fabry Disease Cardiomyopathy
Abstract
Background: The limited ability of enzyme replacement therapy (ERT) in removing globotriaosylceramide from cardiomyocytes is recognized for advanced Fabry disease cardiomyopathy (FDCM). Prehypertrophic FDCM is believed to be cured or stabilized by ERT. However, no pathologic confirmation is available. We report here on the long-term clinical-pathologic impact of ERT on prehypertrophic FDCM.
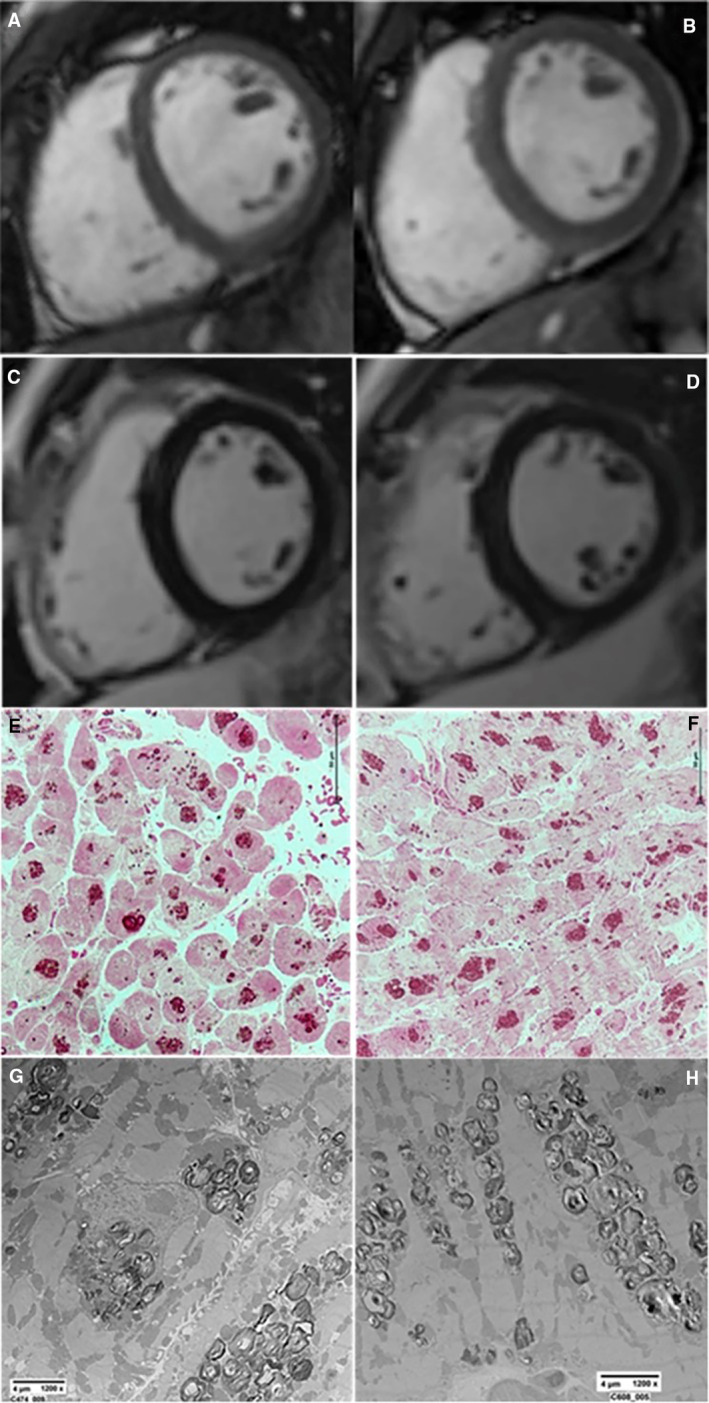
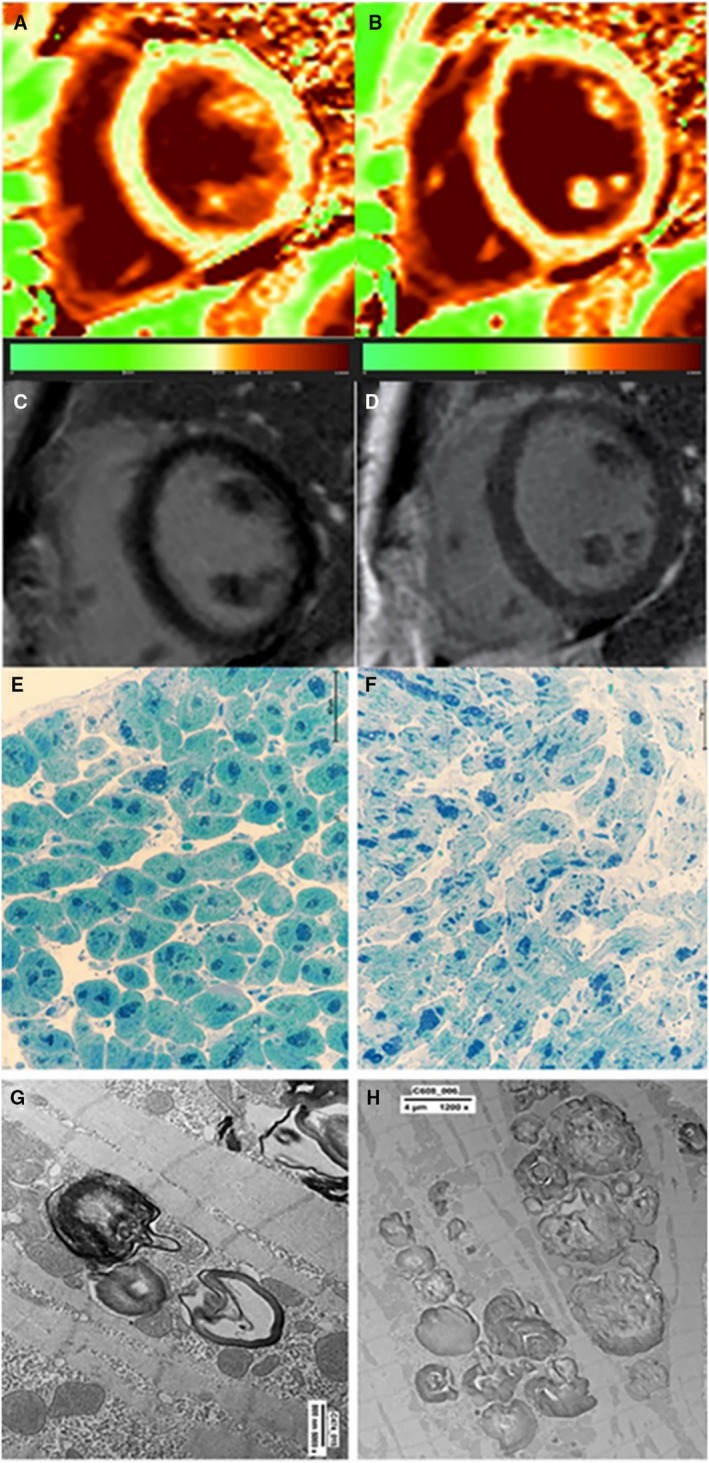
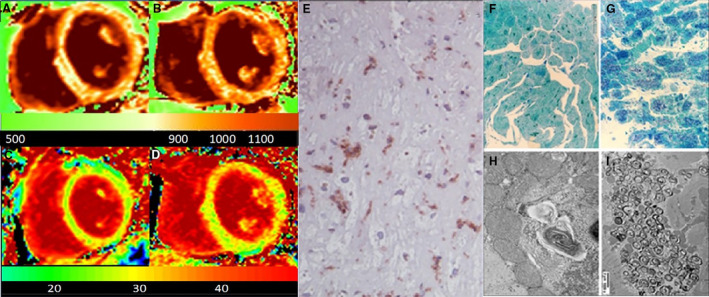
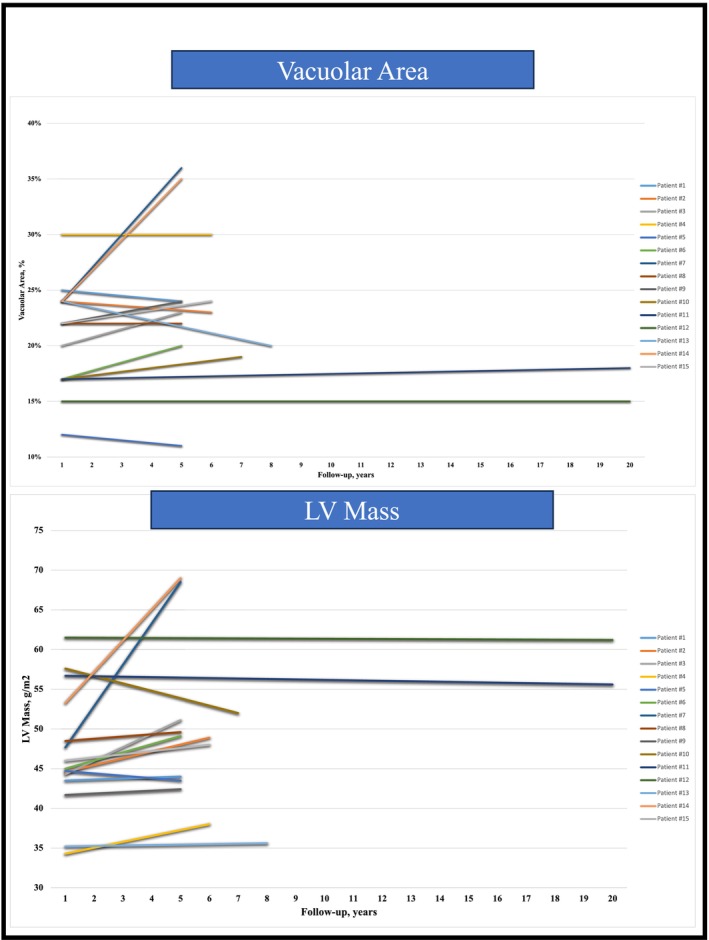
Methods and results: Fifteen patients with Fabry disease with left ventricular maximal wall thickness ≤10.5 mm at cardiac magnetic resonance required endomyocardial biopsy because of angina and ventricular arrhythmias. Endomyocardial biopsy showed coronary small-vessel disease in the angina cohort, and vacuoles in smooth muscle cells and cardiomyocytes ≈20% of the cell surface containing myelin bodies at electron microscopy. Patients received α-agalsidase in 8 cases, and β-agalsidase in 7 cases. Both groups experienced symptom improvement except 1 patients treated with α-agalsidase and 1 treated with β-agalsidase. After ERT administration ranging from 4 to 20 years, all patients had control cardiac magnetic resonance and left ventricular endomyocardial biopsy because of persistence of symptoms or patient inquiry on disease resolution. In 13 asymptomatic patients with FDCM, left ventricular maximal wall thickness and left ventricular mass, cardiomyocyte diameter, vacuole surface/cell surface ratio, and vessels remained unchanged or minimally increased (left ventricular mass increased by <2%) even after 20 years of observation, and storage material was still present at electron microscopy. In 2 symptomatic patients, FDCM progressed, with larger and more engulfed by globotriaosylceramide myocytes being associated with myocardial virus-negative lymphocytic inflammation.
Conclusions: ERT stabilizes storage deposits and myocyte dimensions in 87% of patients with prehypertrophic FDCM. Globotriaosylceramide is never completely removed even after long-term treatment. Immune-mediated myocardial inflammation can overlap, limiting ERT activity.
Keywords: Fabry disease cardiomyopathy; enzyme replacement therapy; globotrioasylceramide; mannose‐6‐phosphate receptors.
Figures
References
-
- Desnick RJ, Brady R, Barranger J, Collins AJ, Germain DP, Goldman M, Grabowski G, Packman S, Wilcox WR. Fabry disease, an under‐recognized multisystemic disorder: expert recommendations for diagnosis, management, and enzyme replacement therapy. Ann Intern Med. 2003;138:338–346. - PubMed
-
- Desnick RJ. Fabry disease (α‐galactosidase A deficiency). Genetic Diseases of the Kidney. Elsevier; 2009:597–616.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
