

Repurposing mebendazole against triple-negative breast cancer CNS metastasis
- PMID: 38563850
- PMCID: PMC11093727
- DOI: 10.1007/s11060-024-04654-x
Repurposing mebendazole against triple-negative breast cancer CNS metastasis
Abstract
Purpose: Triple-negative breast cancer (TNBC) often metastasizes to the central nervous system (CNS) and has the highest propensity among breast cancer subtypes to develop leptomeningeal disease (LMD). LMD is a spread of cancer into leptomeningeal space that speeds up the disease progression and severely aggravates the prognosis. LMD has limited treatment options. We sought to test whether the common anti-helminthic drug mebendazole (MBZ) may be effective against murine TNBC LMD.
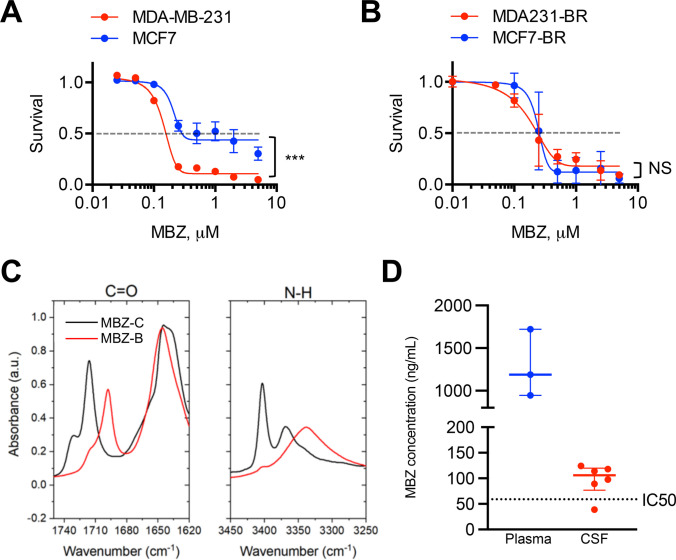
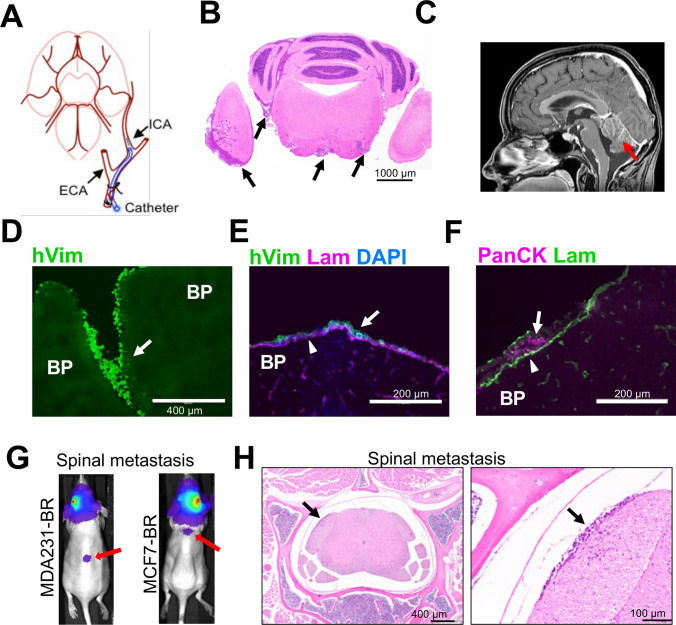
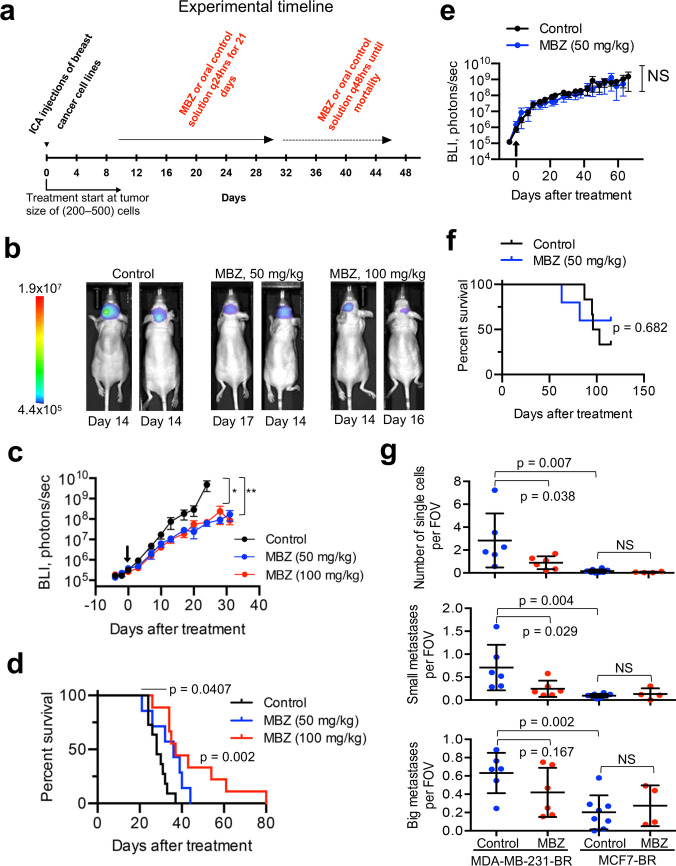
Methods: A small-molecule screen involving TNBC cell lines identified benzimidazoles as potential therapeutic agents for further study. In vitro migration assays were used to evaluate cell migration capacity and the effect of MBZ. For in vivo testing, CNS metastasis was introduced into BALB/c athymic nude mice through internal carotid artery injections of brain-tropic MDA-MB-231-BR or MCF7-BR cells. Tumor growth and spread was monitored by bioluminescence imaging and immunohistochemistry. MBZ was given orally at 50 and 100 mg/kg doses. MBZ bioavailability was assayed by mass spectrometry.
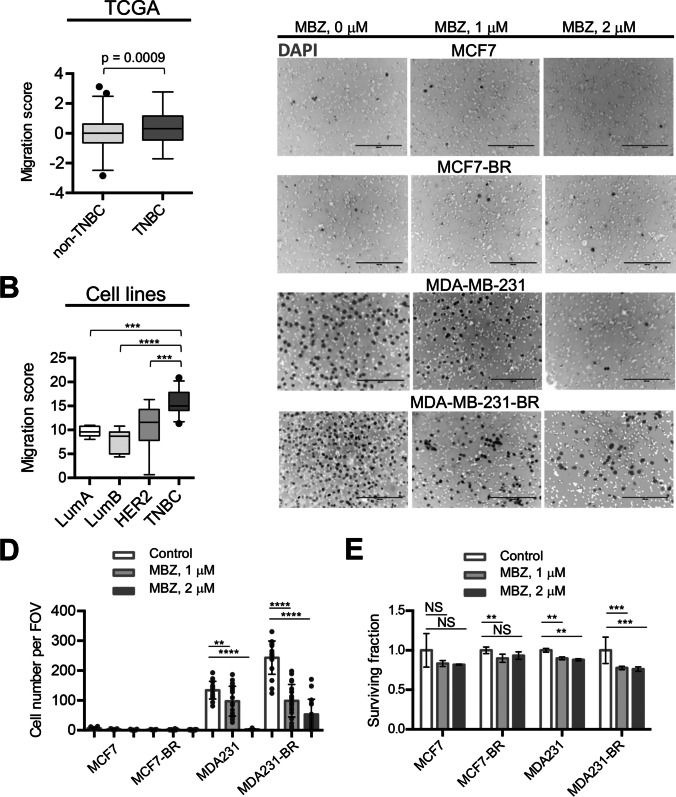
Results: Bioinformatic analysis and migration assays revealed higher migratory capacity of TNBC compared to other breast cancer subtypes. MBZ effectively slowed down migration of TNBC cell line MDA-MB-231 and its brain tropic derivative MDA-MB-231-BR. In animal studies, MBZ reduced leptomeningeal spread, and extended survival in brain metastasis model produced by MDA-MB-231-BR cells. MBZ did not have an effect in the non-migratory MCF7-BR model.
Conclusions: We demonstrated that MBZ is a safe and effective oral agent in an animal model of TNBC CNS metastasis. Our findings are concordant with previous efforts involving MBZ and CNS pathology and support the drug's potential utility to slow down leptomeningeal spread.
Keywords: Breast cancer; Drug repurposing; Leptomeningeal disease; Mebendazole.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Update of
-
Repurposing mebendazole against triple-negative breast cancer leptomeningeal disease.Res Sq [Preprint]. 2024 Feb 5:rs.3.rs-3915392. doi: 10.21203/rs.3.rs-3915392/v1. Res Sq. 2024. Update in: J Neurooncol. 2024 May;168(1):125-138. doi: 10.1007/s11060-024-04654-x. PMID: 38405839 Free PMC article. Updated. Preprint.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
