

Activating Point Mutations in the MET Kinase Domain Represent a Unique Molecular Subset of Lung Cancer and Other Malignancies Targetable with MET Inhibitors
- PMID: 38564707
- PMCID: PMC11294820
- DOI: 10.1158/2159-8290.CD-23-1217
Activating Point Mutations in the MET Kinase Domain Represent a Unique Molecular Subset of Lung Cancer and Other Malignancies Targetable with MET Inhibitors
Abstract
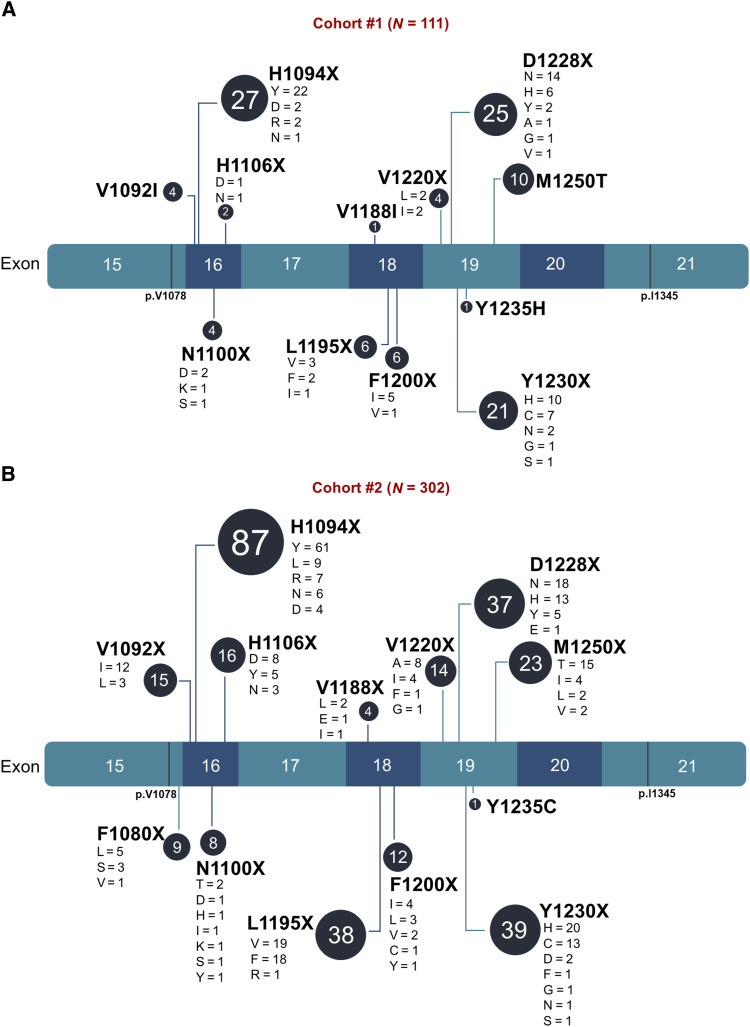
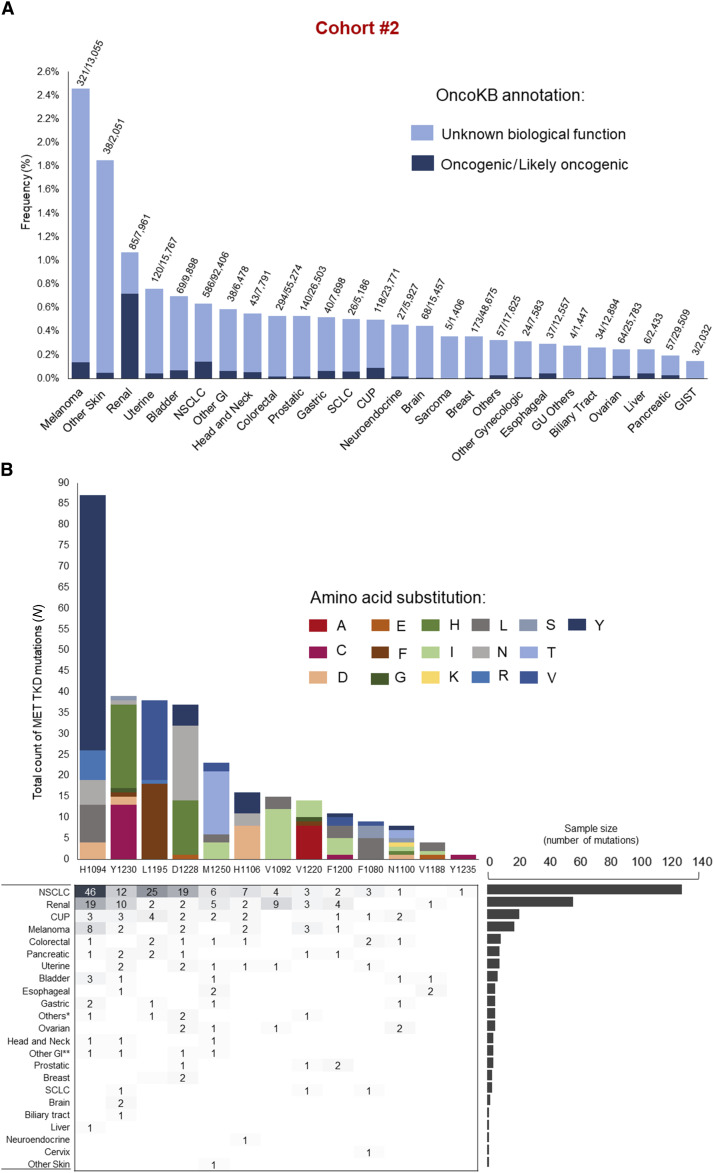
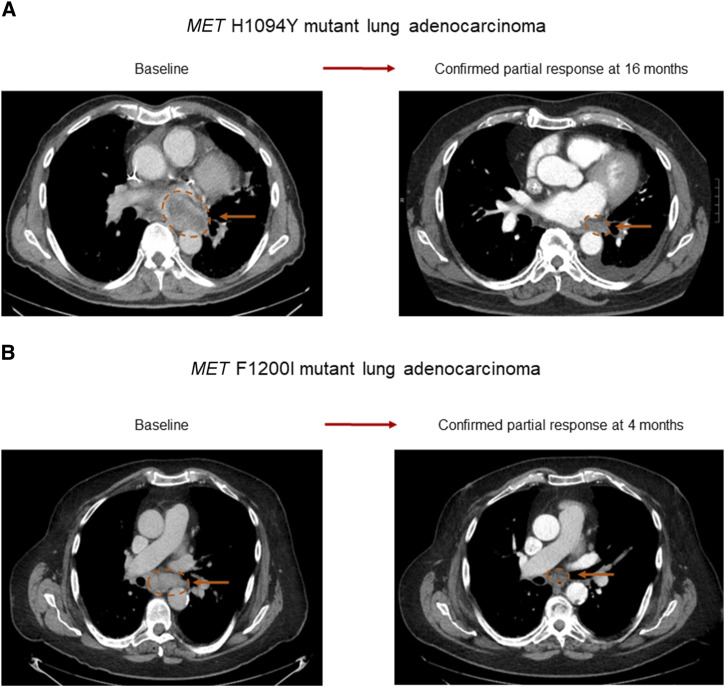
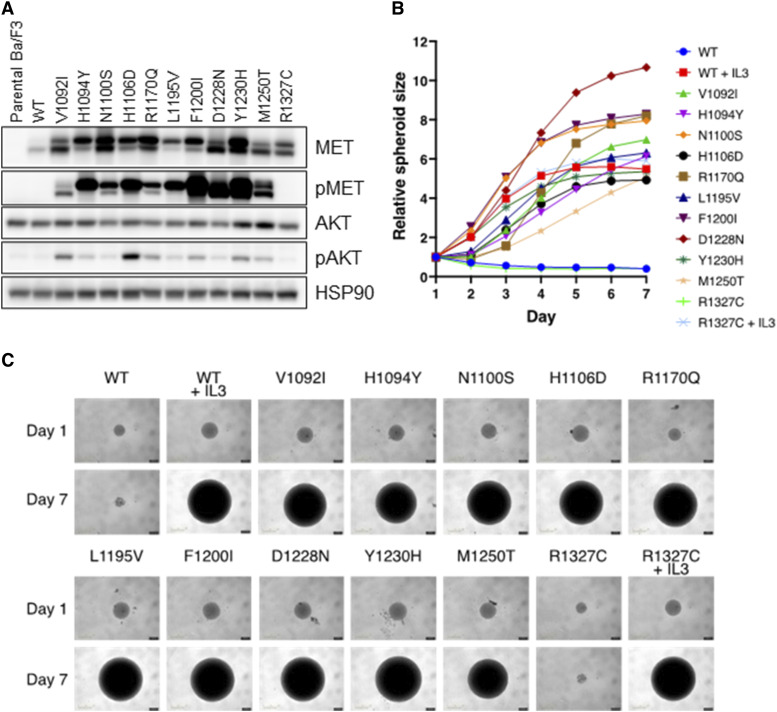
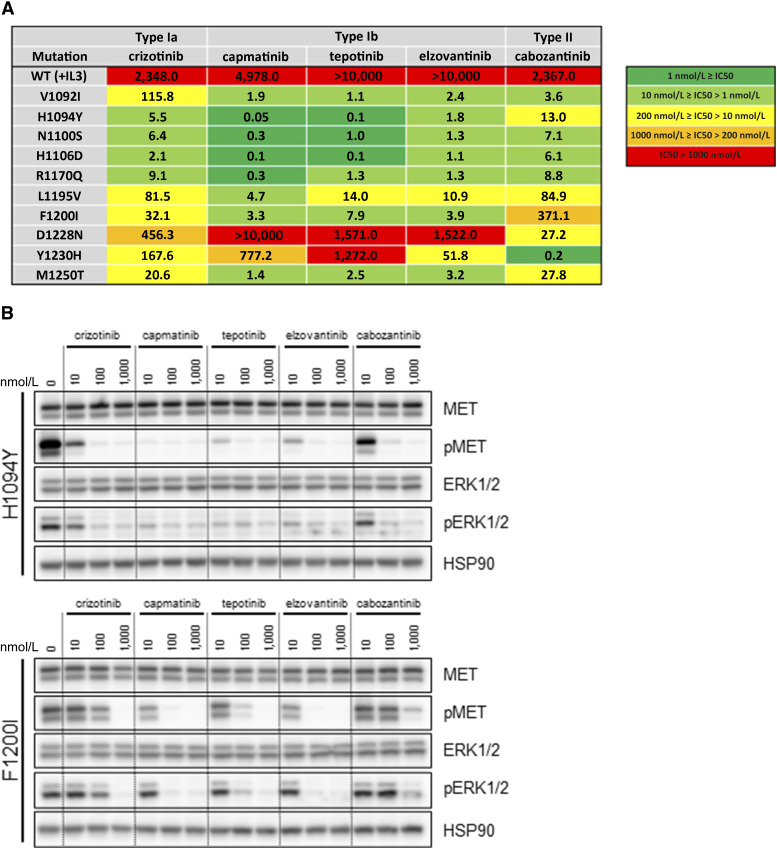
Activating point mutations in the MET tyrosine kinase domain (TKD) are oncogenic in a subset of papillary renal cell carcinomas. Here, using comprehensive genomic profiling among >600,000 patients, we identify activating MET TKD point mutations as putative oncogenic driver across diverse cancers, with a frequency of ∼0.5%. The most common mutations in the MET TKD defined as oncogenic or likely oncogenic according to OncoKB resulted in amino acid substitutions at positions H1094, L1195, F1200, D1228, Y1230, M1250, and others. Preclinical modeling of these alterations confirmed their oncogenic potential and also demonstrated differential patterns of sensitivity to type I and type II MET inhibitors. Two patients with metastatic lung adenocarcinoma harboring MET TKD mutations (H1094Y, F1200I) and no other known oncogenic drivers achieved confirmed partial responses to a type I MET inhibitor. Activating MET TKD mutations occur in multiple malignancies and may confer clinical sensitivity to currently available MET inhibitors. Significance: The identification of targetable genomic subsets of cancer has revolutionized precision oncology and offers patients treatments with more selective and effective agents. Here, we demonstrate that activating, oncogenic MET tyrosine kinase domain mutations are found across a diversity of cancer types and are responsive to MET tyrosine kinase inhibitors.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
S. Nakazawa reports a Research Fellowship from Daiichi Sankyo Foundation of Life Science. B. Ricciuti reports personal fees from AstraZeneca and Regeneron; and personal fees from Amgen outside the submitted work. G. Harada reports personal fees from BMS, Merck, and J&J; personal fees and other support from MSD, AstraZeneca, Lilly, and Takeda; and personal fees from Daiichi Sankyo outside the submitted work. J.K. Lee reports personal fees from Foundation Medicine and Roche during the conduct of the study. J.V. Alessi reports other support from AstraZeneca outside the submitted work. A. Di Federico reports personal fees from Hanson-Wade outside the submitted work. S. Baldacci reports non-financial support from Lilly, GSK, Roche, Pfizer, and Janssen; grants from Intergroupe Francophone de Cancérologie Thoracique and Lille University; personal fees from Boehringer Ingelheim; personal fees and non-financial support from MSD; and personal fees from AstraZeneca outside the submitted work. M.F. Chen reports grants from NCI and ASCO; other support from Nordisk, Quest, and DOCS; and other support from FIGS outside the submitted work. Z. Zimmerman reports other support from Turning Point Therapeutics during the conduct of the study. R.S. Heist reports other support from AbbVie, AstraZeneca, Daichii Sankyo, Claim, Lilly, Novartis, Merck, Sanofi, and Regeneron; grants from Daichii Sankyo, Lilly, Mirati, Novartis, Erasca, Mythic, AbbVie, Agios, and Corvus; and grants from Turning Point outside the submitted work. A. Elliott reports personal fees from Caris Life Sciences outside the submitted work. A.M. Vanderwalde reports other support from Caris Life Sciences during the conduct of the study; other support from George Clinical outside the submitted work. B. Halmos reports grants and personal fees from AstraZeneca, Merck, Boehringer Ingelheim, Pfizer, Janssen, Daiichi, AbbVie, Amgen, Takeda, and BMS; grants from GSK, Advaxis, Black Diamond, Forward Pharma, and Arrivent; personal fees from Genentech; and personal fees from Precede outside the submitted work. S.V. Liu reports grants and personal fees from AbbVie, AstraZeneca, Bristol-Myers Squibb, Elevation Oncology, Genentech, Gilead, Merck, Merus, RAPT, and Turning Point Therapeutics; personal fees from Amgen, Boehringer Ingelheim, Catalyst, Daiichi Sankyo, Guardant Health, Janssen, Jazz Pharmaceuticals, Mirati, Novartis, Pfizer, Regeneron Revolution Medicines, Sanofi, Takeda, grants from Alkermes, Ellipses, Nuvalent, OSE Immunotherapeutics, Puma; and personal fees from Candel Therapeutics outside the submitted work. J. Che reports a scientific cofounder for Matchpoint therapeutics and M3 bioinformatics & Technology Inc. He is an equity holder and scientific consultant for Matchpoint, Allorion, and Soltego. A.B. Schrock reports personal fees from Foundation Medicine and Roche during the conduct of the study. A. Drilon reports personal fees from 14ner/Elevation Oncology, Amgen, AbbVie, ArcherDX, AstraZeneca, Beigene, BergenBio, Blueprint Medicines, Chugai Pharmaceutical, EcoR1, EMD Serono, Entos, Exelixis, Helsinn, Hengrui Therapeutics, Ignyta/Genentech/Roche, Janssen, Loxo/Bayer/Lilly, Merus, Monopteros, MonteRosa, Novartis, Nuvalent, Pfizer, Prelude, Repare RX, Takeda/Ariad/Millenium, Treeline Bio, TP Therapeutics, Tyra Biosciences, Verastem during the conduct of the study; other support from Foundation Medicine, Teva, Taiho, GlaxSmithKlein, other support from mBrace, Treeline, other support from Boehringer Ingelheim, Merck, Puma, and personal fees from Wolters Kluwer, UpToDate outside the submitted work; in addition, A. Drilon has a patent for Selpercatinib-Osimertinib (filed/pending) pending; and CME Honoraria: Answers in CME, Applied Pharmaceutical Science, Inc., AXIS, Clinical Care Options, EPG Health, Harborside Nexus, I3 Health, Imedex, Liberum, Medendi, Medscape, Med Learning, MJH Life Sciences, MORE Health, Ology, OncLive, Paradigm, Peerview Institute, PeerVoice, Physicians Education Resources, Remedica Ltd., Research to Practice, RV More, Targeted Oncology, TouchIME, WebMD. P.A. Jänne reports grants and personal fees from AstraZeneca, Boehringher Ingelheim, Eli Lilly, and Daiichi Sankyo; personal fees from Pfizer, Roche/Genentech, Chugai Pharmaceuticals, SFJ Pharmaceuticals, Voronoi, Biocartis, Novartis, Sanofi Oncology, Takeda Oncology, Mirati Therapeutics, Transcenta, Silicon Therapeutics, Syndax, Nuvalent, Bayer, Eisai, Allorion Therapeutics, Accutar Biotech, AbbVie, Mone Rosa, Scorpion Therapeutics, Merus, Frontier Medicines, Hongyun Biotechnology, Duality Biologics, and Blueprint Medicines; grants from PUMA and REvolution Medicines outside the submitted work; in addition, P.A. Jänne has a patent for EGFR mutations issued and licensed to Lab Corp. M.M. Awad reports personal fees from Genmab, Janssen, Genentech, Merck, Novartis, Mirati, and Blueprint; grants and personal fees from Bristol-Myers Squibb and AstraZeneca; grants from Amgen; and grants and personal fees from Lilly during the conduct of the study. No disclosures were reported by the other authors.
Figures
References
-
- Wolf J, Seto T, Han J-Y, Reguart N, Garon EB, Groen HJM, et al. Capmatinib in MET exon 14–mutated or MET-amplified non–small-cell lung cancer. N Engl J Med 2020;383:944–57. - PubMed
-
- Remon J, Hendriks LEL, Mountzios G, García-Campelo R, Saw SPL, Uprety D, et al. MET alterations in NSCLC—current perspectives and future challenges. J Thorac Oncol 2023;18:419–35. - PubMed
-
- Stella G, Senetta R, Balderacchi A, Cassoni P, Comoglio P, Benvenuti S. Oncogenic potential of MET SEMA mutations affecting brain metastases from NSCLC is sustained by their microrheological features. Eur Respir J 2017;50:PA3306.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
