

Impact of pulmonary hypertension on outcomes after TEER in patients suffering from mitral regurgitation
- PMID: 38565712
- PMCID: PMC11839688
- DOI: 10.1007/s00392-024-02442-1
Impact of pulmonary hypertension on outcomes after TEER in patients suffering from mitral regurgitation
Abstract
Aim: Data on associations of invasively determined hemodynamic parameters with procedural success and outcomes in patients suffering from mitral regurgitation (MR) undergoing transcatheter edge-to-edge repair of the mitral valve (M-TEER) is limited.
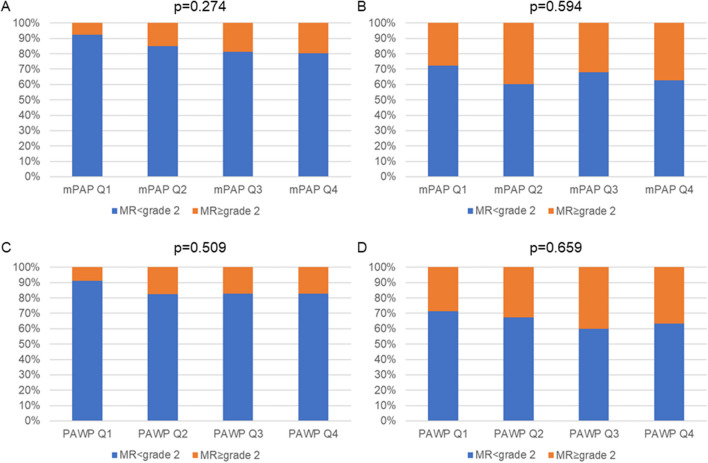
Methods and results: We enrolled 239 patients with symptomatic MR of grade 2 + , who received M-TEER. All patients underwent extensive pre-interventional invasive hemodynamic measurements via right heart catheterization (mean pulmonary arterial pressure (mPAP), systolic- (PAPsys) and diastolic pulmonary arterial pressure (PAPdia), pulmonary arterial wedge pressure (PAWP), a-wave, v-wave, pulmonary vascular resistance (PVR), transpulmonary pressure gradient (TPG), cardiac index (CI), stroke volume index (SVI)). mPAP and PAWP at baseline were neither associated with procedural success, immediate reduction of MR, nor residual MR after 6 months of follow-up. The composite outcome (All-cause mortality (ACM) and/or heart failure induced rehospitalization (HFH)) and HFH differed significantly after M-TEER when stratified according to mPAP, PAWP, PAPdia, a-wave and v-wave. ACM was not associated with the afore mentioned parameters. Neither PVR, TPG, CI nor SVI were associated with the composite outcome and HFH, respectively. In multivariable analyses, PAWP was independently associated with the composite outcome and HFH. PVR and SVI were not associated with outcomes.
Conclusion: PAWP at baseline was significantly and independently associated with HFH and might serve as a valuable parameter for identifying patients at high risk for HFH after M-TEER. ACM and procedural success were not affected by pulmonary arterial pressure before M-TEER. We suggest that the post-capillary component of PH serves as the driving force behind the risk of HFH.
Keywords: Mitral valve transcatheter edge-to-edge repair; Outcome Assessment; Pulmonary Arterial Hypertension.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: The authors have no conflicts of interest to disclose.
Figures



Similar articles
-
Association of pulmonary hypertension with the outcome in patients undergoing edge-to-edge mitral valve repair.Heart. 2024 May 10;110(11):800-807. doi: 10.1136/heartjnl-2023-323473. Heart. 2024. PMID: 38388469
-
Impact of Updated Invasive Right Ventricular and Pulmonary Hemodynamics on Long-Term Outcomes in Patients With Mitral Valve Transcatheter Edge-to-Edge Repair.Am J Cardiol. 2025 Jan 1;234:99-106. doi: 10.1016/j.amjcard.2024.11.010. Epub 2024 Nov 21. Am J Cardiol. 2025. PMID: 39572265
-
Clinical Outcomes of Mitral Regurgitation Severity and Transcatheter Edge-to-Edge Repair in Atrial Functional Mitral Regurgitation.Catheter Cardiovasc Interv. 2025 Jul;106(1):494-503. doi: 10.1002/ccd.31567. Epub 2025 May 4. Catheter Cardiovasc Interv. 2025. PMID: 40320723
-
Outcomes of mitral valve transcatheter edge-to-edge repair for patients with hemodynamic instability: A systematic review and meta-analysis.Cardiovasc Revasc Med. 2024 Oct;67:19-28. doi: 10.1016/j.carrev.2024.04.006. Epub 2024 Apr 4. Cardiovasc Revasc Med. 2024. PMID: 38584083
-
Transcatheter Edge-to-Edge Repair for Severe Mitral Regurgitation in Patients With Cardiogenic Shock: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2025 Mar 18;14(6):e034932. doi: 10.1161/JAHA.124.034932. Epub 2025 Mar 7. J Am Heart Assoc. 2025. PMID: 40055145 Free PMC article.
Cited by
-
The impact of pulmonary hypertension on prognosis in moderate-to-severe mitral regurgitation patients treated with transcatheter edge-to-edge mitral valve repair: a comprehensive meta-analysis.Front Cardiovasc Med. 2025 Jan 10;11:1489674. doi: 10.3389/fcvm.2024.1489674. eCollection 2024. Front Cardiovasc Med. 2025. PMID: 39866800 Free PMC article.
References
-
- Stone GW, Lindenfeld J, Abraham WT, Kar S, Lim DS, Mishell JM et al (2018) Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N Engl J Med 379(24):2307–2318. 10.1056/NEJMoa1806640 - PubMed
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F et al (2021) 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 143(5):e72–e227. 10.1161/CIR.0000000000000923 - PubMed
-
- Geisler T, Jorbenadze R, Popov AF, Mueller KL, Rath D, Droppa M et al (2019) Thrombogenicity and Antithrombotic Strategies in Structural Heart Interventions and Nonaortic Cardiac Device Therapy-Current Evidence and Practice. Thromb Haemost 119(10):1590–1605. 10.1055/s-0039-1694751 - PubMed
-
- Kar S, Feldman T, Qasim A, Trento A, Kapadia S, Pedersen W et al (2019) Five-year outcomes of transcatheter reduction of significant mitral regurgitation in high-surgical-risk patients. Heart 105(21):1622–1628. 10.1136/heartjnl-2017-312605 - PubMed
-
- Lombard FW, Liang Y (2019) Risk Factors for Mitral Valve Surgery: Atrial Fibrillation and Pulmonary Hypertension. Semin Cardiothorac Vasc Anesth 23(1):57–69. 10.1177/1089253218821694 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
