

Preoperative Gallows traction as an adjunct to hip open reduction surgery: Is it safe and is it effective?
- PMID: 38567049
- PMCID: PMC10984156
- DOI: 10.1177/18632521241229620
Preoperative Gallows traction as an adjunct to hip open reduction surgery: Is it safe and is it effective?
Abstract
Background: Traction is used at our hospital before open reduction in infants with developmental dysplasia of the hip. Theoretically, it reduces soft-tissue tension, allowing an easier surgical reduction and therefore lower surgical complications. Owing to extended hospital stays, potential complications, and lack of evidence, the use of traction has decreased. This study aims to quantify whether traction is safe and whether it has any demonstrable effect.
Methods: The perioperative course of 80 patients undergoing preoperative traction and hip open reduction were reviewed. The height of hip dislocation was classified using the International Hip Dysplasia Institute classification system on both radiographs taken before and after traction. Any complications related to traction were recorded, along with the requirement for femoral shortening osteotomies, incidence of re-dislocation, and longer-term rate of avascular necrosis.
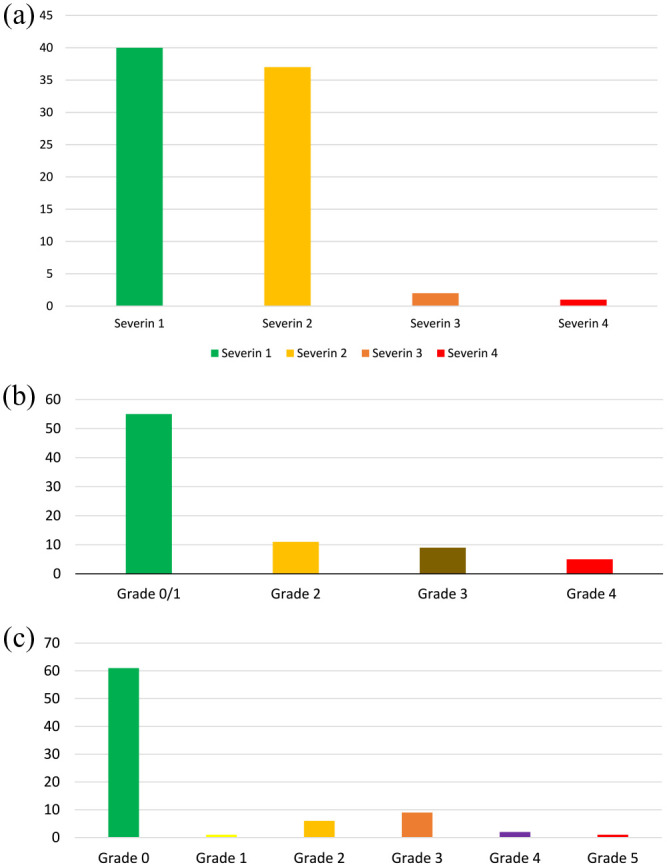
Results: Traction lowered the resting position of the majority of hips, with the median International Hip Dysplasia Institute grade before traction improving from 4 to 3, a statistically significant improvement (p < 0.00001). There were no neurovascular complications. Two babies were complicated with broken skin sores; however, surgery still progressed uneventfully. Zero hips in the cohort required femoral shortening osteotomies to achieve a tension-free reduction, and the re-dislocation rate was 0%. However, 96% of hips were Severin 1 or 2 at 6-year follow-up.
Conclusion: Notably, 1 week of preoperative traction significantly improves the resting position of the hip in high dislocations. It is safe when used in infants weighing <12 kg, and subsequent surgical outcomes are excellent, thus supporting its use ahead of developmental dysplasia of the hip open reduction surgery.
Level of evidence: Level IV.
Keywords: Developmental dysplasia of the hip; Gallows traction; avascular necrosis; preoperative traction.
© The Author(s) 2024.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures




References
-
- Hunter JB. Femoral shaft fractures in children. Injury 2005; 36(Suppl. 1): A86–A93. - PubMed
-
- Holmes SJ, Sedgwick DM, Scobie WG. Domiciliary gallows traction for femoral shaft fractures in young children. Feasibility, safety and advantages. J Bone Joint Surg Br 1983; 65(3): 288–290. - PubMed
-
- Rampal V, Sabourin M, Erdeneshoo E, et al.. Closed reduction with traction for developmental dysplasia of the hip in children aged between one and five years. J Bone Joint Surg Br 2008; 90(7): 858–863. - PubMed
-
- Salter RB, Kostuik J, Dallas S. Avascular necrosis of the femoral head as a complication of treatment for congenital dislocation of the hip in young children: a clinical and experimental investigation. Can J Surg 1969; 12(1): 44–61. - PubMed
-
- Fogarty EE, Accardo NJ., Jr. Incidence of avascular necrosis of the femoral head in congenital hip dislocation related to the degree of abduction during preliminary traction. J Pediatr Orthop 1981; 1(3): 307–311. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
