

Prognostic Value of Right Ventricular Afterload in Patients Undergoing Mitral Transcatheter Edge-to-Edge Repair
- PMID: 38567665
- PMCID: PMC11262498
- DOI: 10.1161/JAHA.123.033510
Prognostic Value of Right Ventricular Afterload in Patients Undergoing Mitral Transcatheter Edge-to-Edge Repair
Abstract
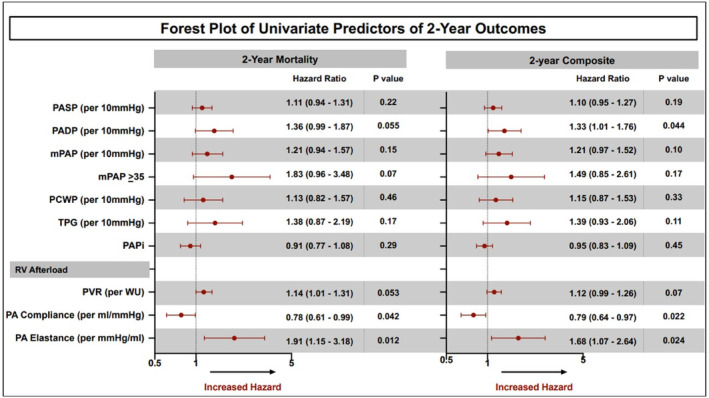
Background: Pulmonary hypertension (PH) and secondary mitral regurgitation (MR) are associated with adverse outcomes after mitral transcatheter edge-to-edge repair. We aim to study the prognostic value of invasively measured right ventricular afterload in patients undergoing mitral transcatheter edge-to-edge repair.
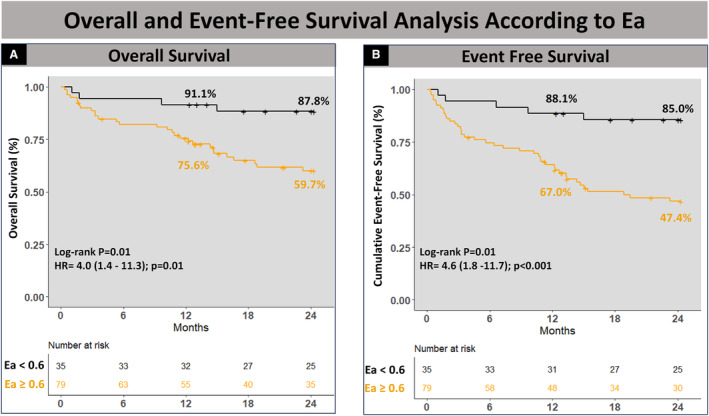
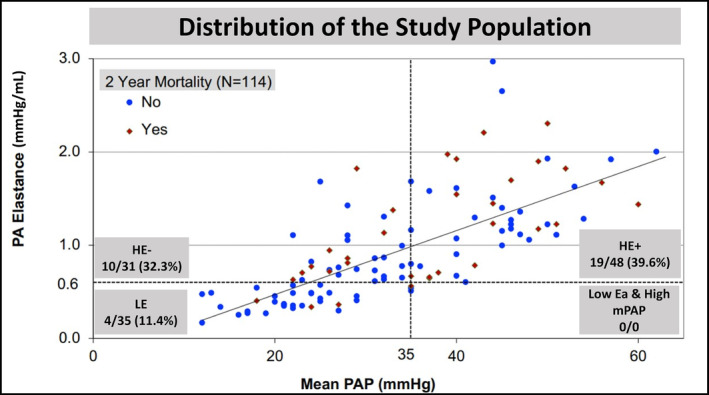
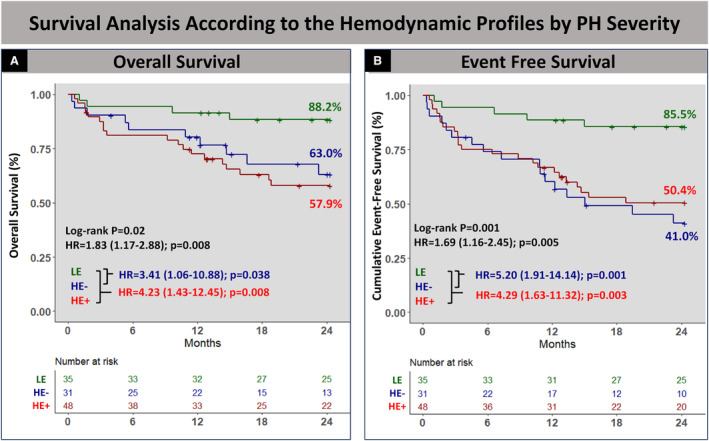
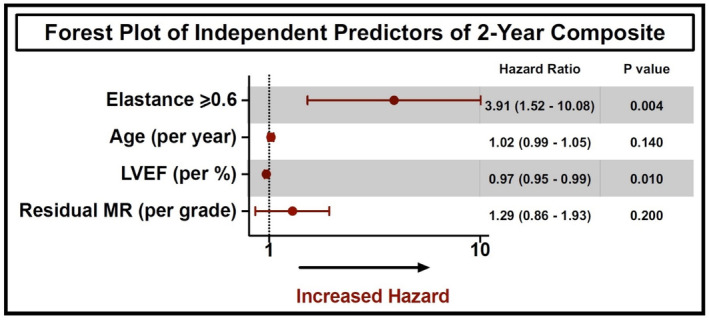
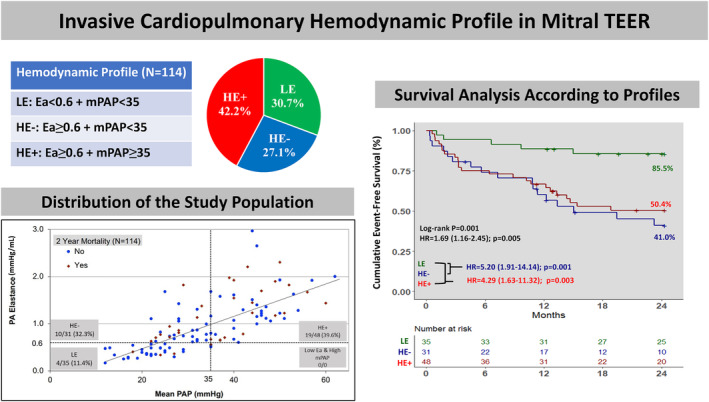
Methods and results: We identified patients who underwent right heart catheterization ≤1 month before transcatheter edge-to-edge repair. The end points were all-cause mortality and a composite of mortality and heart failure hospitalization at 2 years. Using the receiver operating characteristic curve-derived threshold of 0.6 for pulmonary effective arterial elastance ([Ea], pulmonary artery systolic pressure/stroke volume), patients were stratified into 3 profiles based on PH severity (low elastance [HE]: Ea <0.6/mean pulmonary artery pressure (mPAP)) <35; High Elastance with No/Mild PH (HE-): Ea ≥0.6/mPAP <35; and HE with Moderate/Severe PH (HE+): Ea ≥0.6/mPAP ≥35) and MR pathogenesis (Primary MR [PMR])/low elastance, PMR/HE, and secondary MR). The association between this classification and clinical outcomes was examined using Cox regression. Among 114 patients included, 50.9% had PMR. Mean±SD age was 74.7±10.6 years. Patients with Ea ≥0.6 were more likely to have diabetes, atrial fibrillation, New York Heart Association III/IV status, and secondary MR (all P<0.05). Overall, 2-year cumulative survival was 71.1% and was lower in patients with secondary MR and mPAP ≥35. Compared with patients with low elastance, cumulative 2-year event-free survival was significantly lower in HE- and HE+ patients (85.5% versus 50.4% versus 41.0%, respectively, P=0.001). Also, cumulative 2-year event-free survival was significantly higher in patients with PMR/low elastance when compared with PMR/HE and patients with secondary mitral regurgitation (85.5% versus 55.5% versus 46.1%, respectively, P=0.005).
Conclusions: Assessment of the preprocedural cardiopulmonary profile based on mPAP, MR pathogenesis, and Ea guides patient selection by identifying hemodynamic features that indicate likely benefit from mitral-transcatheter edge-to-edge repair in PH or lack thereof.
Keywords: mitral regurgitation; mitral transcatheter edge‐to‐edge repair; pulmonary effective arterial elastance; pulmonary hypertension; right ventricular afterload.
Figures
Comment in
-
It's All About That Right Ventricle.J Am Heart Assoc. 2024 Apr 16;13(8):e034711. doi: 10.1161/JAHA.124.034711. Epub 2024 Apr 3. J Am Heart Assoc. 2024. PMID: 38567674 Free PMC article. No abstract available.
References
-
- Bursi F, Barbieri A, Grigioni F, Reggianini L, Zanasi V, Leuzzi C, Ricci C, Piovaccari G, Branzi A, Modena MG. Prognostic implications of functional mitral regurgitation according to the severity of the underlying chronic heart failure: a long‐term outcome study. Eur J Heart Fail. 2010;12:382–388. doi: 10.1093/eurjhf/hfq014 - DOI - PubMed
-
- Ghoreishi M, Evans CF, DeFilippi CR, Hobbs G, Young CA, Griffith BP, Gammie JS. Pulmonary hypertension adversely affects short‐ and long‐term survival after mitral valve operation for mitral regurgitation: implications for timing of surgery. J Thorac Cardiovasc Surg. 2011;142:1439–1452. doi: 10.1016/j.jtcvs.2011.08.030 - DOI - PubMed
-
- Ben‐Yehuda O, Shahim B, Chen S, Liu M, Redfors B, Hahn RT, Asch FM, Weissman NJ, Medvedofsky D, Puri R, et al. Pulmonary hypertension in transcatheter mitral valve repair for secondary mitral regurgitation: the COAPT trial. J Am Coll Cardiol. 2020;76:2595–2606. doi: 10.1016/j.jacc.2020.09.609 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
