

doi: 10.1007/s10388-024-01054-y.
Epub 2024 Apr 3.
Japanese Classification of Esophageal Cancer, 12th Edition: Part I
Affiliations
- PMID: 38568243
- PMCID: PMC11199297
- DOI: 10.1007/s10388-024-01054-y
Item in Clipboard
Japanese Classification of Esophageal Cancer, 12th Edition: Part I
Esophagus.
2024 Jul.
Abstract
This is the first half of English edition of Japanese Classification of Esophageal Cancer, 12th Edition that was published by the Japan Esophageal Society in 2022.
Keywords: Chemotherapy; Endoscopic treatment; Esophageal cancer; Japanese classification; Radiotherapy; Surgery.
© 2024. The Author(s).
Figures
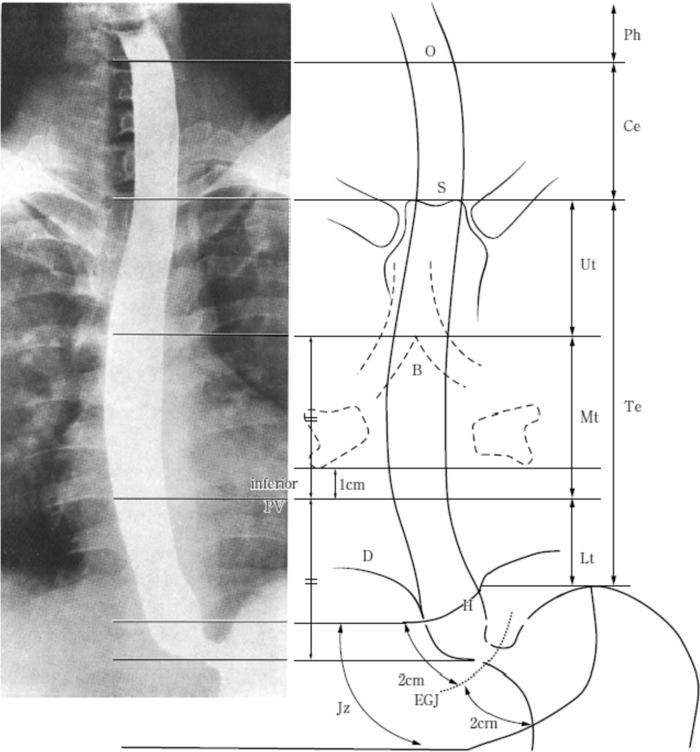
Tumor location. O: esophageal orifice, S: superior margin of the sternum, B: tracheal bifurcation, PV: pulmonary vein, D: diaphragm, EGJ: esophagogastric junction, H: esophageal hiatus
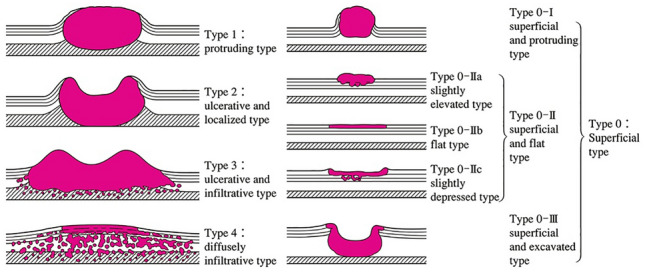
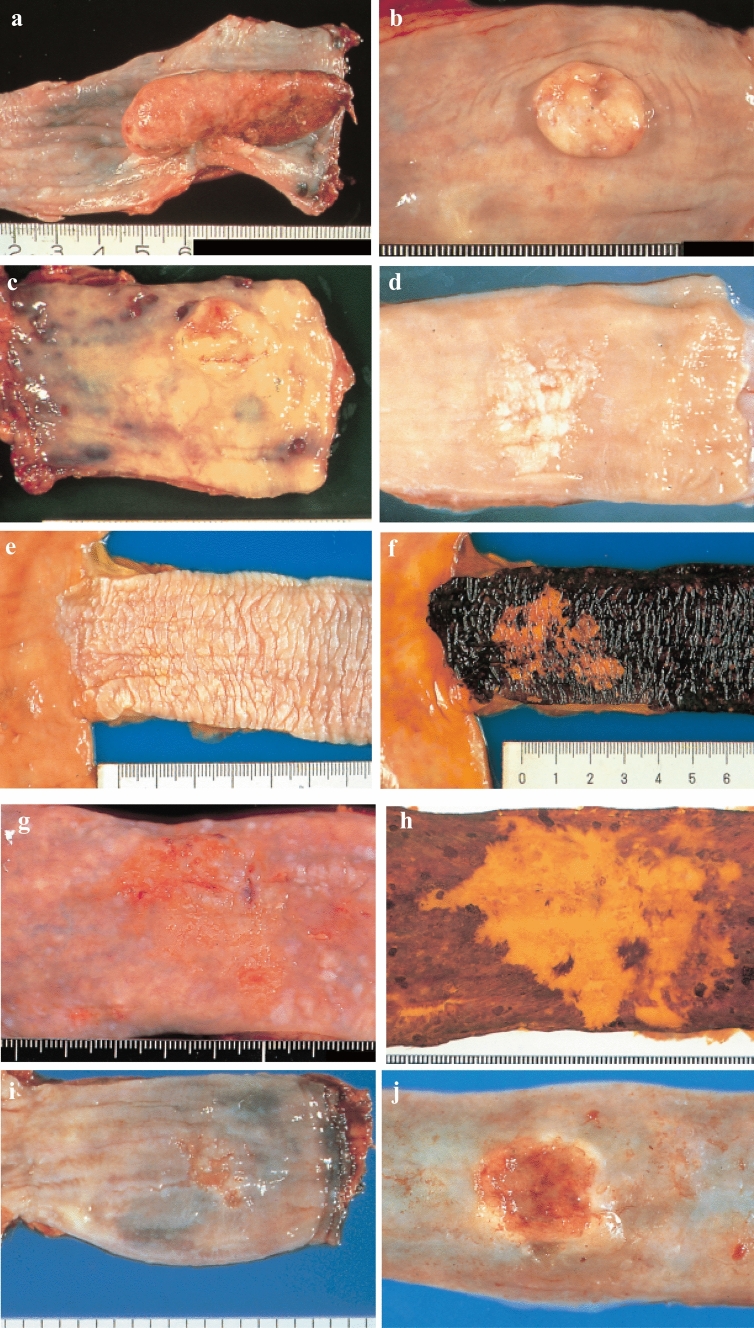
Macroscopic classification (Type 0–4)
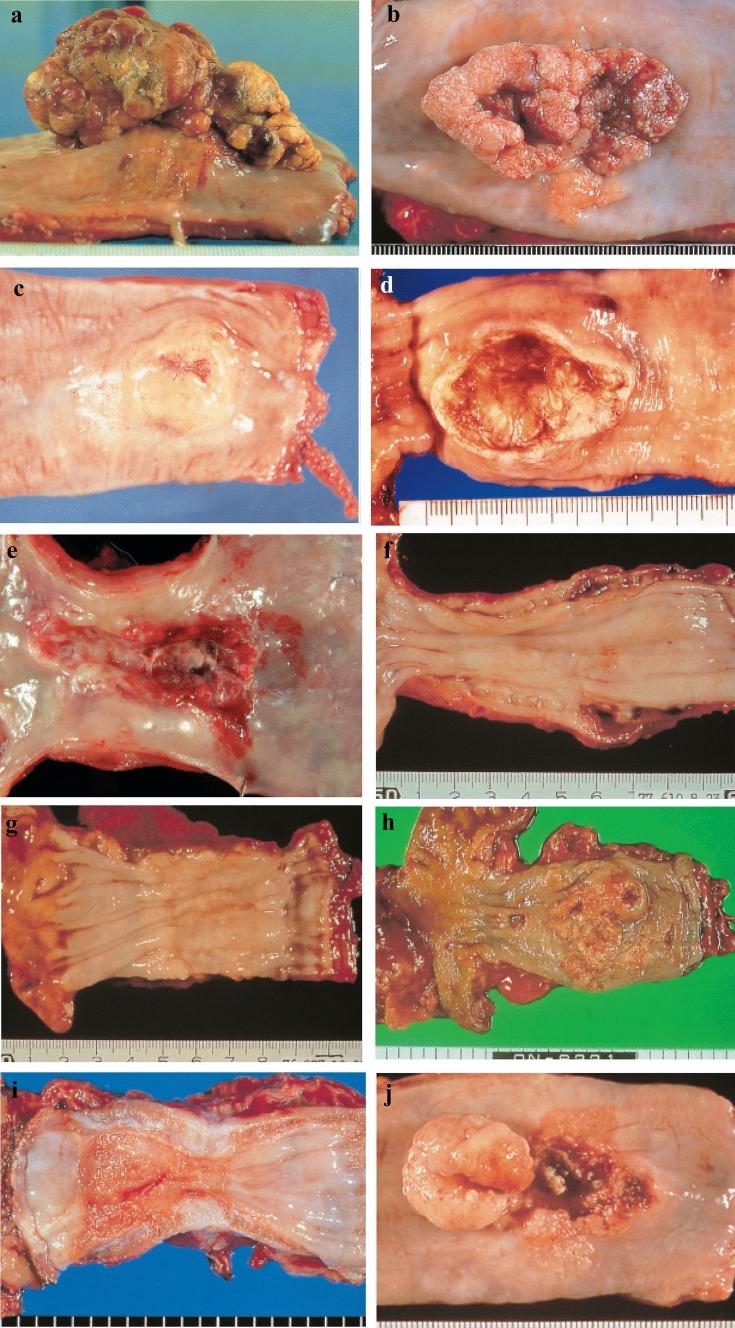
a Type 1: A pedunculated and tall polypoid lesion. This is judged to be advanced cancer based on its size, immobility (or cut cross section). b Type 1: This protruding lesion with a clearly demarcated border has lobules or a papillary appearance on its surface. c Type 1: Most of the surface of the protrusion is covered by non-cancerous epithelium. This is judged to be advanced cancer based on its size and immobility. d Type 2: This lesion is a deep ulcer with a well-demarcated surrounding ridge. e Type 3: This lesion is a deep ulcer surrounded by a poorly demarcated ridge. The lesion extends circumferentially causing luminal stenosis. f Type 4: This diffusely invasive lesion with no clear margin makes the esophageal wall thick and hard and causes luminal stenosis. No distinct ulcer can be seen. g Type 4: The thickening of the esophageal wall and the edematous changes of the mucosa suggest diffuse intramural extension of the lesion, but there is no finding of hardening or stenosis, and no finding of ulcer formation. h Type 5a: The macroscopic appearance is extremely complex with Type 1, and Type 2 and others, and it is difficult to categorize. i Type 5b: This macroscopic tumor (Type 5b) cannot be categorized because of preoperative chemoradiotherapy. j Combined Type. This cancer showed mixed morphology of advanced Type 1, Type 2, and 0-IIc.
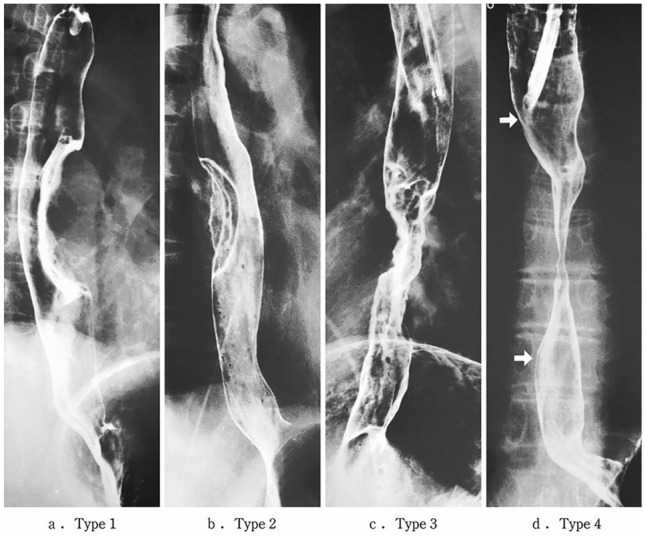
Roentgenological findings advanced type

a-1 Type 1, protruding type (pT2): A tall lesion with a broad base. a-2 Type 1, protruding type (pT2): A tall lesion with a narrow base. b Type 2, ulcerative and localized type (pT3). A deep ulcerative lesion surrounded by a well-demarcated ridge. c Type 3, ulcerative and infiltrative type (pT3). A deep ulcerative lesion surrounded by an ill-demarcated ridge. d Type 4, diffusely infiltrative type (pT3). Ill-defined thickening and hardening of the esophageal wall accompanied by luminal stenosis is observed. There is no remarkable ulcer formation
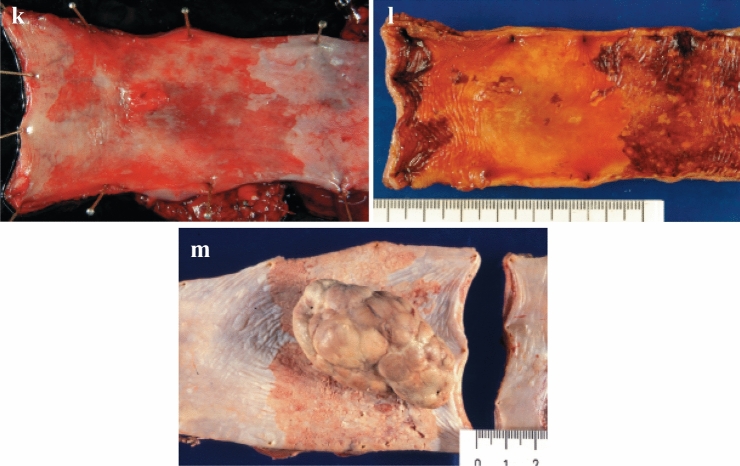
a Type 0-Ip (superficial, protruding type, and pedunculated). The tumor is well demarcated and has a narrow base. b Type 0-Ip (superficial, protruding type and pedunculated). The well-demarcated, protruding tumor has an irregular and nodular surface. c Type 0-Is (superficial protruding type, and sessile). The surface of this ill-demarcated tumor is mostly covered by the normal epithelium. d Type 0-IIa (slightly elevated type). The generally white tumor is only slightly elevated from the mucosa. e Type 0-IIb (Flat type). Only minute irregularities and no macroscopic abnormal features are observed. f Type 0-IIb (Flat type) (Iodine-stained view of e). The superficial tumor is unstained by iodine. g Type 0-IIc (slightly depressed type). The superficial depressed lesion has no clear margin and a finely granular surface. h Type 0-IIc (Iodine-stained view of g) The superficial tumor is unstained by iodine. i Type 0-IIc (slightly depressed type). The superficial depressed lesion has an irregular margin. j Type 0-III (superficial and depressed type). The deeply depressed lesion with a slightly elevated margin suggests invasion beyond the muscularis mucosa. k Type 0-IIc + “0-IIa” (superficial spreading type). The widespread slightly depressed red lesion (0-IIc) has a slightly elevated lesion (0-IIa) in its center, suggesting invasion into the submucosal layer. The lesion, more than 5 cm in length, is defined as the superficial spreading type. l Type 0-IIc + “0-IIa” (superficial spreading type) (Iodine-stained view of k). The reddish depressed lesion is not stained with iodine solution. m Type 0-IIc + “0-Ip”. The well-demarcated protruding tumor with a narrow base (0-Ip) has a slightly depressed lesion (0-IIc) in the surrounding area
a Type 0-Ip (superficial, protruding type, and pedunculated). The tumor is well demarcated and has a narrow base. b Type 0-Ip (superficial, protruding type and pedunculated). The well-demarcated, protruding tumor has an irregular and nodular surface. c Type 0-Is (superficial protruding type, and sessile). The surface of this ill-demarcated tumor is mostly covered by the normal epithelium. d Type 0-IIa (slightly elevated type). The generally white tumor is only slightly elevated from the mucosa. e Type 0-IIb (Flat type). Only minute irregularities and no macroscopic abnormal features are observed. f Type 0-IIb (Flat type) (Iodine-stained view of e). The superficial tumor is unstained by iodine. g Type 0-IIc (slightly depressed type). The superficial depressed lesion has no clear margin and a finely granular surface. h Type 0-IIc (Iodine-stained view of g) The superficial tumor is unstained by iodine. i Type 0-IIc (slightly depressed type). The superficial depressed lesion has an irregular margin. j Type 0-III (superficial and depressed type). The deeply depressed lesion with a slightly elevated margin suggests invasion beyond the muscularis mucosa. k Type 0-IIc + “0-IIa” (superficial spreading type). The widespread slightly depressed red lesion (0-IIc) has a slightly elevated lesion (0-IIa) in its center, suggesting invasion into the submucosal layer. The lesion, more than 5 cm in length, is defined as the superficial spreading type. l Type 0-IIc + “0-IIa” (superficial spreading type) (Iodine-stained view of k). The reddish depressed lesion is not stained with iodine solution. m Type 0-IIc + “0-Ip”. The well-demarcated protruding tumor with a narrow base (0-Ip) has a slightly depressed lesion (0-IIc) in the surrounding area

a Type 0-Ip, superficial, protruding type, and pedunculated (cT1b-SM2-3). A well-demarcated protruding and pedunculated tumor shows an irregular and nodular surface. b Type 0-Is, Superficial and protruding type, sessile (pT1b-SM2). A well-demarcated protruding and sessile tumor. c Type 0-Is, superficial, protruding type, and sessile (pT1b-SM2). 1 Conventional endoscopy: An ill-demarcated protruding tumor covered by normal esophageal mucosa suggests a tumor mass in the submucosa. 2 Iodine staining: The mucosa covering the tumor is stained brown, and an unstained area at the top suggests exposed tumor tissue. d Type 0-IIa, slightly elevated type (pT1a-MM). A plaque-like, slightly elevated white tumor. Tumor invasion of the white area remains within the lamina propria, while a tiny protrusion at the distal margin of the tumor invades the muscularis mucosa. e Type 0-IIa, slightly elevated type (pT1a-EP). A slightly elevated tumor with well-demarcated reddening (the height of a type 0-IIa lesion is less than 1 mm). f Type 0-IIb flat type (pT1a-EP). 1 Conventional endoscopy: A conventional observation cannot detect the lesion. 2 Narrow band imaging: A brownish area can be detected. 3 Iodine staining: A completely flat lesion is identified as a well-demarcated, unstained area using iodine staining. g Type 0-IIc, slightly depressed type (pT1a-LPM). 1 Conventional endoscopy: An irregularly shaped mucosal reddening with a slight depression is visible. 2 Narrow band imaging: The lesion is also visible as a brownish area. 3 Iodine staining: A well-demarcated, unstained area is visible using iodine staining. h Type 0-IIc, slightly depressed type (pT1b-SM1). 1 Conventional endoscopy: An area of mucosal reddening with a slight depression and marginal elevation is visible. 2 Narrow band imaging: A brownish area suggesting a hypervascular lesion is visible. i Type 0-III, Superficial and excavated type (cT1b-SM2-3). 1 Conventional endoscopy: A distinctly depressed lesion with a surrounding elevated area is visible, suggesting an ulcer reaching the muscularis mucosa. 2 Narrow band imaging: A well-demarked lesion with surrounding elevated area is visible as a brownish area. j Combined type 0-IIc + ”0-Is” (pT1b-SM2). 1 Conventional endoscopy: A distinct elevation with a wider base is visible. A slightly depressed lesion close to the distal margin is also observed. 2 Narrow band imaging: A lesion with a well-demarcated margin is visible. k Combined type 0-Is + 0- IIc (pT1b-SM2). 1 Conventional endoscopy: A distinctly protruding lesion with a wide base and irregular nodular changes is visible. Reddening of the esophageal mucosa close to the lesion with an ill-defined margin is suspected. 2 Iodine staining: The margin of the mucosal change is identified as well-demarcated, unstained area

a Type 0-Ip, superficial, protruding type, and pedunculated (cT1b-SM2-3). A well-demarcated protruding and pedunculated tumor shows an irregular and nodular surface. b Type 0-Is, Superficial and protruding type, sessile (pT1b-SM2). A well-demarcated protruding and sessile tumor. c Type 0-Is, superficial, protruding type, and sessile (pT1b-SM2). 1 Conventional endoscopy: An ill-demarcated protruding tumor covered by normal esophageal mucosa suggests a tumor mass in the submucosa. 2 Iodine staining: The mucosa covering the tumor is stained brown, and an unstained area at the top suggests exposed tumor tissue. d Type 0-IIa, slightly elevated type (pT1a-MM). A plaque-like, slightly elevated white tumor. Tumor invasion of the white area remains within the lamina propria, while a tiny protrusion at the distal margin of the tumor invades the muscularis mucosa. e Type 0-IIa, slightly elevated type (pT1a-EP). A slightly elevated tumor with well-demarcated reddening (the height of a type 0-IIa lesion is less than 1 mm). f Type 0-IIb flat type (pT1a-EP). 1 Conventional endoscopy: A conventional observation cannot detect the lesion. 2 Narrow band imaging: A brownish area can be detected. 3 Iodine staining: A completely flat lesion is identified as a well-demarcated, unstained area using iodine staining. g Type 0-IIc, slightly depressed type (pT1a-LPM). 1 Conventional endoscopy: An irregularly shaped mucosal reddening with a slight depression is visible. 2 Narrow band imaging: The lesion is also visible as a brownish area. 3 Iodine staining: A well-demarcated, unstained area is visible using iodine staining. h Type 0-IIc, slightly depressed type (pT1b-SM1). 1 Conventional endoscopy: An area of mucosal reddening with a slight depression and marginal elevation is visible. 2 Narrow band imaging: A brownish area suggesting a hypervascular lesion is visible. i Type 0-III, Superficial and excavated type (cT1b-SM2-3). 1 Conventional endoscopy: A distinctly depressed lesion with a surrounding elevated area is visible, suggesting an ulcer reaching the muscularis mucosa. 2 Narrow band imaging: A well-demarked lesion with surrounding elevated area is visible as a brownish area. j Combined type 0-IIc + ”0-Is” (pT1b-SM2). 1 Conventional endoscopy: A distinct elevation with a wider base is visible. A slightly depressed lesion close to the distal margin is also observed. 2 Narrow band imaging: A lesion with a well-demarcated margin is visible. k Combined type 0-Is + 0- IIc (pT1b-SM2). 1 Conventional endoscopy: A distinctly protruding lesion with a wide base and irregular nodular changes is visible. Reddening of the esophageal mucosa close to the lesion with an ill-defined margin is suspected. 2 Iodine staining: The margin of the mucosal change is identified as well-demarcated, unstained area

a Type 0-Ip, superficial, protruding type, and pedunculated (cT1b-SM2-3). A well-demarcated protruding and pedunculated tumor shows an irregular and nodular surface. b Type 0-Is, Superficial and protruding type, sessile (pT1b-SM2). A well-demarcated protruding and sessile tumor. c Type 0-Is, superficial, protruding type, and sessile (pT1b-SM2). 1 Conventional endoscopy: An ill-demarcated protruding tumor covered by normal esophageal mucosa suggests a tumor mass in the submucosa. 2 Iodine staining: The mucosa covering the tumor is stained brown, and an unstained area at the top suggests exposed tumor tissue. d Type 0-IIa, slightly elevated type (pT1a-MM). A plaque-like, slightly elevated white tumor. Tumor invasion of the white area remains within the lamina propria, while a tiny protrusion at the distal margin of the tumor invades the muscularis mucosa. e Type 0-IIa, slightly elevated type (pT1a-EP). A slightly elevated tumor with well-demarcated reddening (the height of a type 0-IIa lesion is less than 1 mm). f Type 0-IIb flat type (pT1a-EP). 1 Conventional endoscopy: A conventional observation cannot detect the lesion. 2 Narrow band imaging: A brownish area can be detected. 3 Iodine staining: A completely flat lesion is identified as a well-demarcated, unstained area using iodine staining. g Type 0-IIc, slightly depressed type (pT1a-LPM). 1 Conventional endoscopy: An irregularly shaped mucosal reddening with a slight depression is visible. 2 Narrow band imaging: The lesion is also visible as a brownish area. 3 Iodine staining: A well-demarcated, unstained area is visible using iodine staining. h Type 0-IIc, slightly depressed type (pT1b-SM1). 1 Conventional endoscopy: An area of mucosal reddening with a slight depression and marginal elevation is visible. 2 Narrow band imaging: A brownish area suggesting a hypervascular lesion is visible. i Type 0-III, Superficial and excavated type (cT1b-SM2-3). 1 Conventional endoscopy: A distinctly depressed lesion with a surrounding elevated area is visible, suggesting an ulcer reaching the muscularis mucosa. 2 Narrow band imaging: A well-demarked lesion with surrounding elevated area is visible as a brownish area. j Combined type 0-IIc + ”0-Is” (pT1b-SM2). 1 Conventional endoscopy: A distinct elevation with a wider base is visible. A slightly depressed lesion close to the distal margin is also observed. 2 Narrow band imaging: A lesion with a well-demarcated margin is visible. k Combined type 0-Is + 0- IIc (pT1b-SM2). 1 Conventional endoscopy: A distinctly protruding lesion with a wide base and irregular nodular changes is visible. Reddening of the esophageal mucosa close to the lesion with an ill-defined margin is suspected. 2 Iodine staining: The margin of the mucosal change is identified as well-demarcated, unstained area

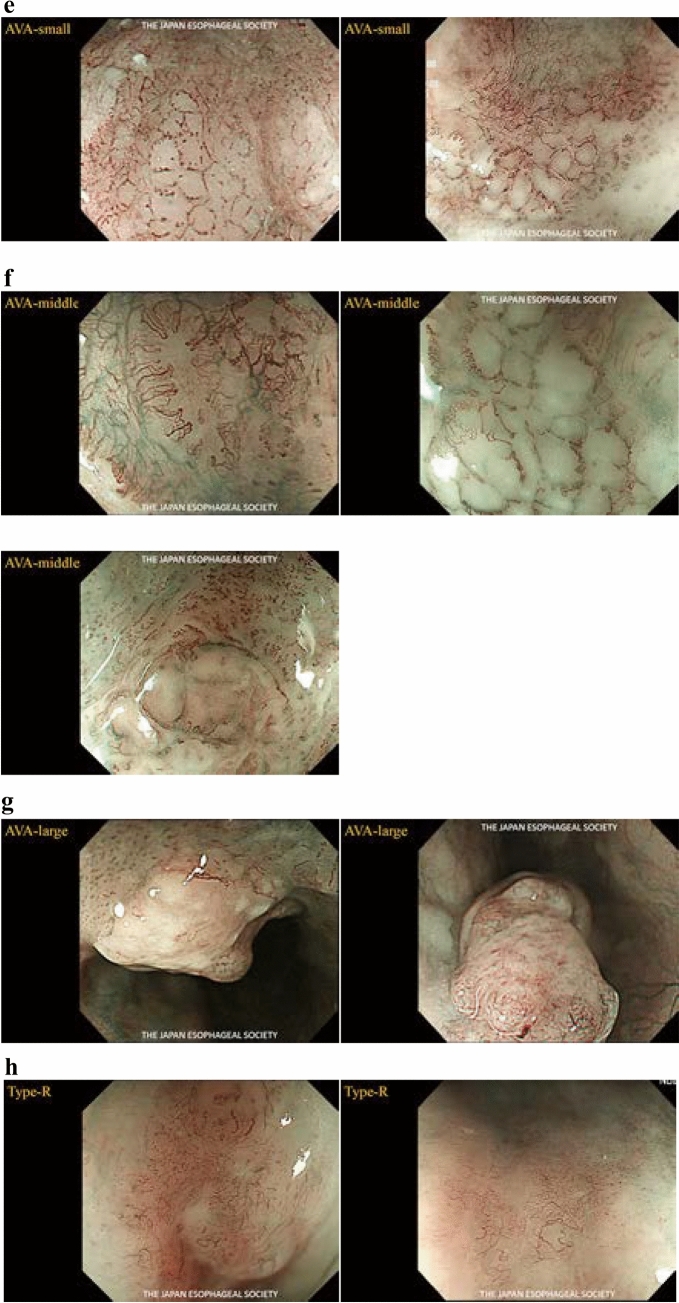
Subclassification for superficial cancer
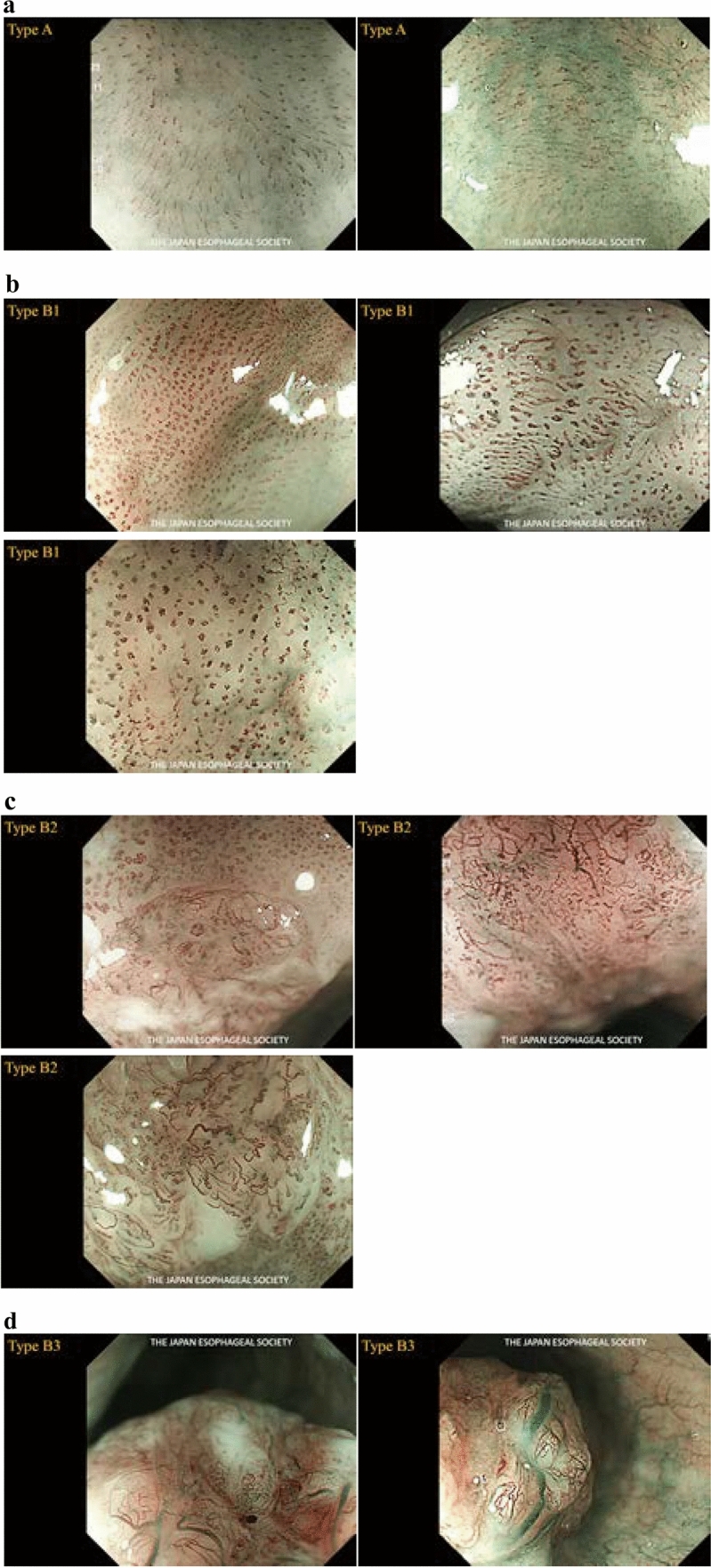
a Type A. b Type B1. c Type B2. d Type B3. e AVA‒small. f AVA‒middle. g AVA‒large. h Type R
a Type A. b Type B1. c Type B2. d Type B3. e AVA‒small. f AVA‒middle. g AVA‒large. h Type R

Cases of the primary lesion contacting the trachea. a Type 2, circumference, and posterior wall. b Type 2, circumference, and posterior wall. c Type 2, 2/3 of the circumference, and left-anterior wall

Cases of the primary lesion contacting the left main bronchus. a Type 2, circumference, and posterior wall. b Type 1, circumference, and left wall. c Type 2, circumference, and posterior wall

Cases contacting the aorta. a Type 3, 1/3 of the circumference, and right wall. b Type 2, 2/3 of the circumference, and right wall. c Type 2, sub-circumference, and right wall

a and b A case whose invasion to the aorta is not ruled out (a and b are of the same case)

a and b A case whose invasion to the aorta is not ruled out (a and b are of the same case)

a and b A case whose invasion to the trachea is not ruled out (a and b are of the same case)

a and b A case with suspicion of invasion to the left main bronchus (a and b are of the same case)

a and b Cases with invasions to the trachea

a–c Cases with invasions to the left main bronchus

a–d Cases with invasions to the trachea from metastatic lymph nodes

a and b Cases with invasions to the aorta

a and b Cases with invasions to the aorta from metastatic lymph nodes

Tumor size and the distance from resection margin to tumor. a Greatest longitudinal dimension (mm). b Greatest transverse dimension (mm)
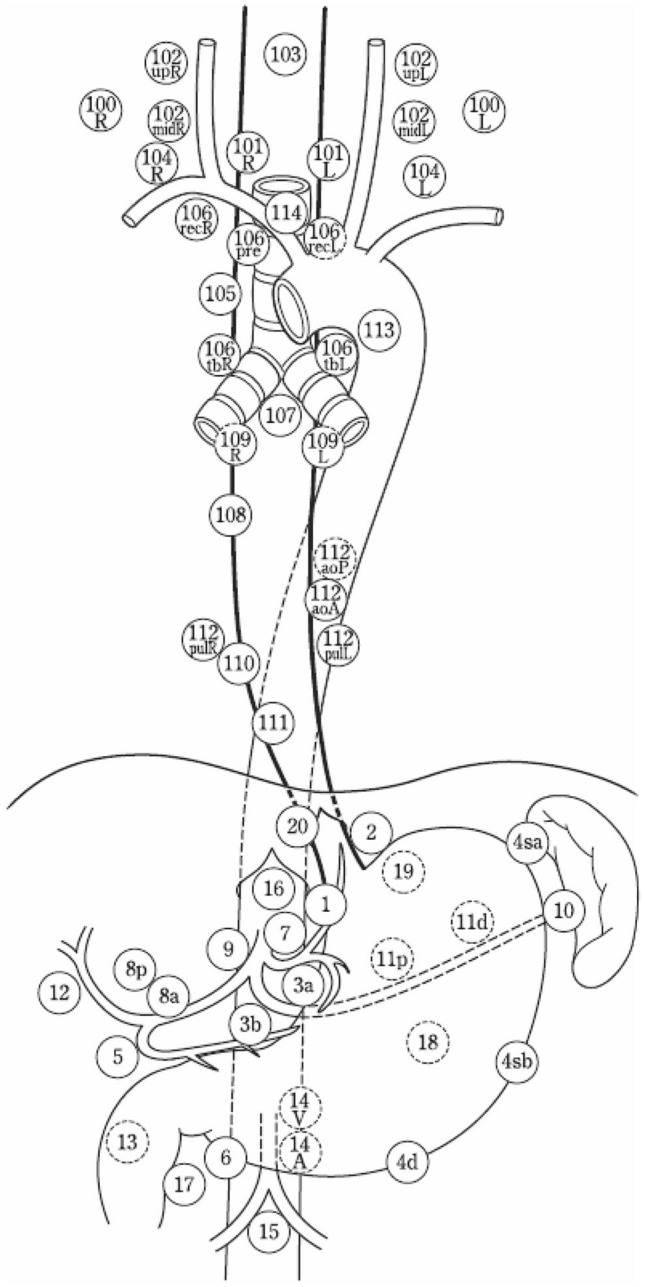
Station numbers of regional lymph nodes

Regional lymph nodes of cervical esophageal cancer (Ce)

Regional lymph nodes of thoracic esophageal cancer (Te)

Regional lymph nodes of zone of esophagogastric junction cancer (Jz)

How to cut endoscopically resected specimens

How to cut surgically resected specimens
References
-
- Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. 8. New York: Wiley-Blackwell; 2017.
-
- Oyama T, Momma K, Makuuchi H. Japan esophageal society classification of superficial esophageal squamous cell carcinoma (in Japanese) Endosc Dig. 2012;24:466–468.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical