

Integrated Hepatitis C-Opioid Use Disorder Care Through Facilitated Telemedicine: A Randomized Trial
- PMID: 38568601
- PMCID: PMC10993166
- DOI: 10.1001/jama.2024.2452
Integrated Hepatitis C-Opioid Use Disorder Care Through Facilitated Telemedicine: A Randomized Trial
Abstract
Importance: Facilitated telemedicine may promote hepatitis C virus elimination by mitigating geographic and temporal barriers.
Objective: To compare sustained virologic responses for hepatitis C virus among persons with opioid use disorder treated through facilitated telemedicine integrated into opioid treatment programs compared with off-site hepatitis specialist referral.
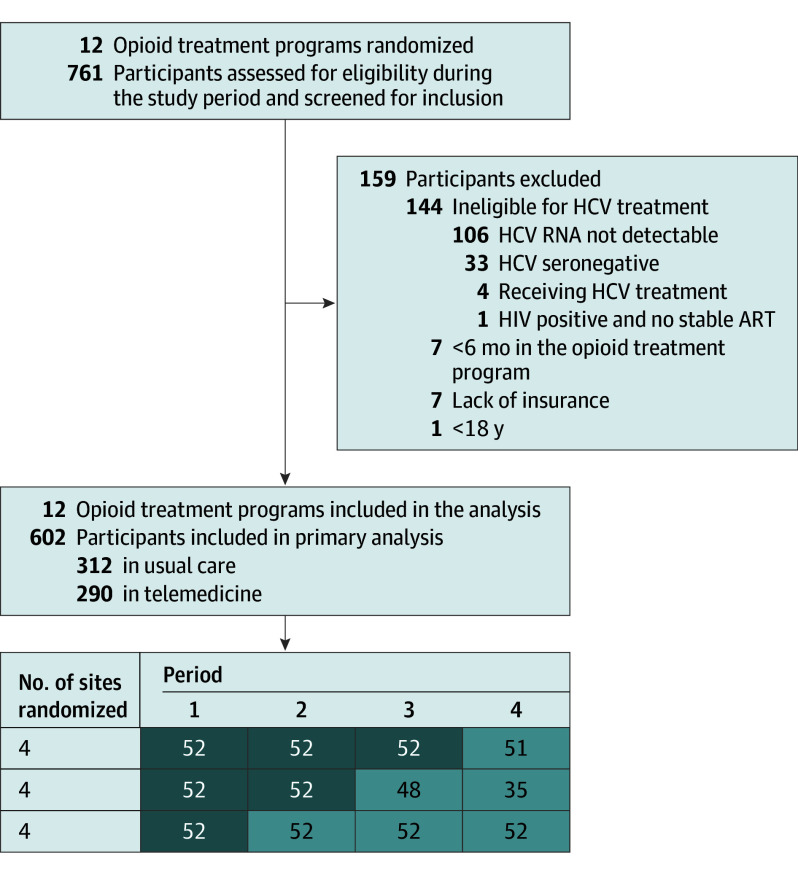
Design, setting, and participants: Prospective, cluster randomized clinical trial using a stepped wedge design. Twelve programs throughout New York State included hepatitis C-infected participants (n = 602) enrolled between March 1, 2017, and February 29, 2020. Data were analyzed from December 1, 2022, through September 1, 2023.
Intervention: Hepatitis C treatment with direct-acting antivirals through comanagement with a hepatitis specialist either through facilitated telemedicine integrated into opioid treatment programs (n = 290) or standard-of-care off-site referral (n = 312).
Main outcomes and measures: The primary outcome was hepatitis C virus cure. Twelve programs began with off-site referral, and every 9 months, 4 randomly selected sites transitioned to facilitated telemedicine during 3 steps without participant crossover. Participants completed 2-year follow-up for reinfection assessment. Inclusion criteria required 6-month enrollment in opioid treatment and insurance coverage of hepatitis C medications. Generalized linear mixed-effects models were used to test for the intervention effect, adjusted for time, clustering, and effect modification in individual-based intention-to-treat analysis.
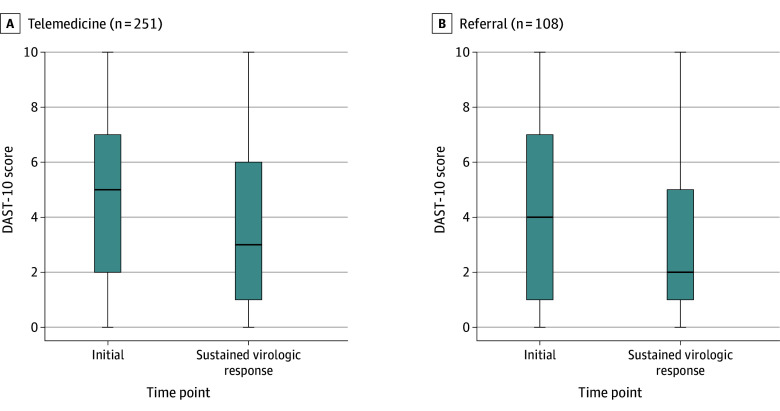
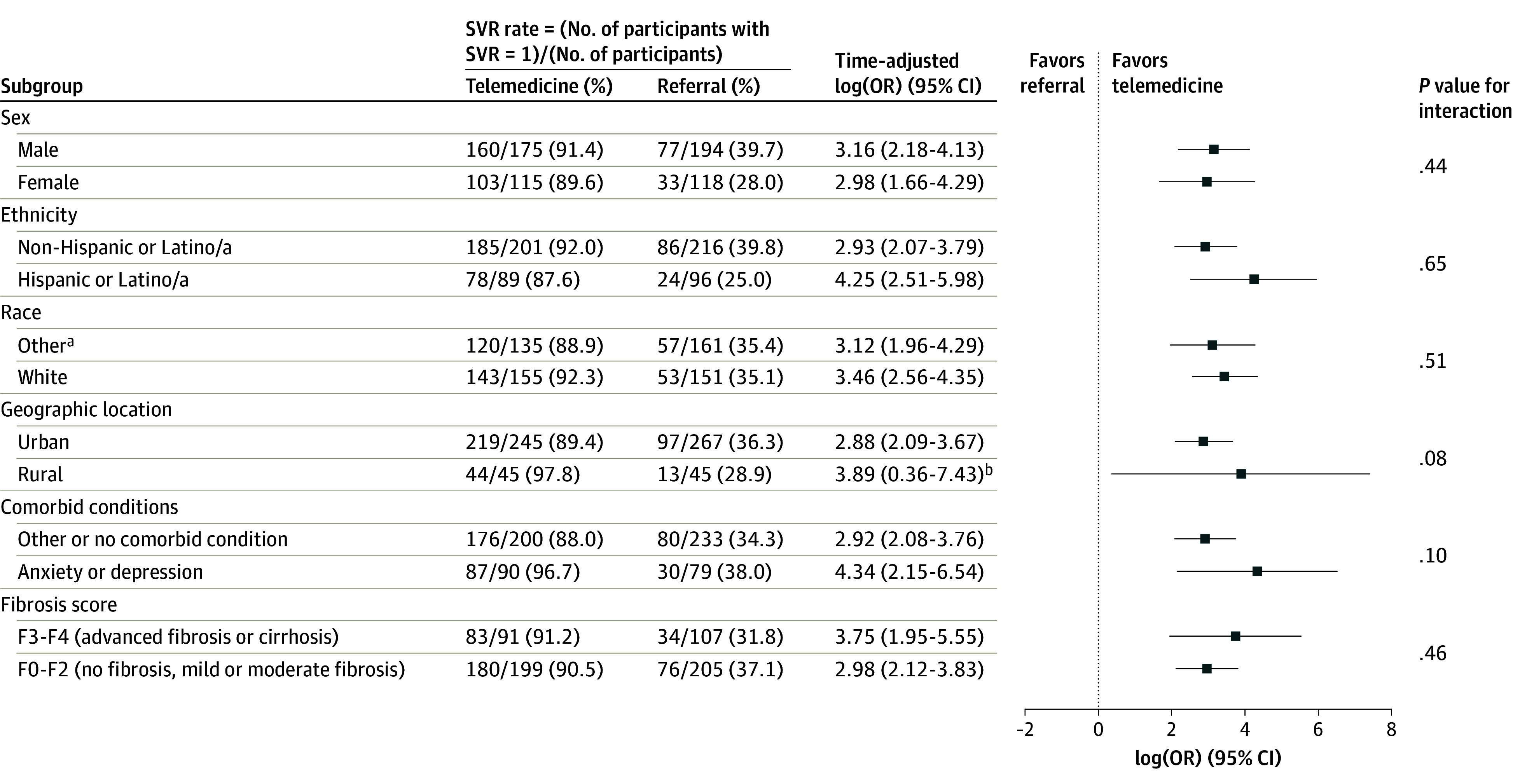
Results: Among 602 participants, 369 were male (61.3%); 296 (49.2%) were American Indian or Alaska Native, Asian, Black or African American, multiracial, or other (ie, no race category was selected, with race data collected according to the 5 standard National Institutes of Health categories); and 306 (50.8%) were White. The mean (SD) age of the enrolled participants in the telemedicine group was 47.1 (13.1) years; that of the referral group was 48.9 (12.8) years. In telemedicine, 268 of 290 participants (92.4%) initiated treatment compared with 126 of 312 participants (40.4%) in referral. Intention-to-treat cure percentages were 90.3% (262 of 290) in telemedicine and 39.4% (123 of 312) in referral, with an estimated logarithmic odds ratio of the study group effect of 2.9 (95% CI, 2.0-3.5; P < .001) with no effect modification. Observed cure percentages were 246 of 290 participants (84.8%) in telemedicine vs 106 of 312 participants (34.0%) in referral. Subgroup effects were not significant, including fibrosis stage, urban or rural participant residence location, or mental health (anxiety or depression) comorbid conditions. Illicit drug use decreased significantly (referral: 95% CI, 1.2-4.8; P = .001; telemedicine: 95% CI, 0.3-1.0; P < .001) among cured participants. Minimal reinfections (n = 13) occurred, with hepatitis C virus reinfection incidence of 2.5 per 100 person-years. Participants in both groups rated health care delivery satisfaction as high or very high.
Conclusions and relevance: Opioid treatment program-integrated facilitated telemedicine resulted in significantly higher hepatitis C virus cure rates compared with off-site referral, with high participant satisfaction. Illicit drug use declined significantly among cured participants with minimal reinfections.
Trial registration: ClinicalTrials.gov Identifier: NCT02933970.
Conflict of interest statement
Figures
References
-
- Daniel H, Bornstein SS, Kane GC, et al. ; Health and Public Policy Committee of the American College of Physicians . Addressing social determinants to improve patient care and promote health equity: an American College of Physicians position paper. Ann Intern Med. 2018;168(8):577-578. doi: 10.7326/M17-2441 - DOI - PubMed
-
- Outland BE, Erickson S, Doherty R, Fox W, Ward L; Medical Practice and Quality Committee of the American College of Physicians . Reforming physician payments to achieve greater equity and value in health care: a position paper of the American College of Physicians. Ann Intern Med. 2022;175(7):1019-1021. doi: 10.7326/M21-4484 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
