

Neuroimaging alterations and relapse in early-stage psychosis
- PMID: 38569725
- PMCID: PMC10980532
- DOI: 10.1503/jpn.230115
Neuroimaging alterations and relapse in early-stage psychosis
Abstract
Background: Recent reports have indicated that symptom exacerbation after a period of improvement, referred to as relapse, in early-stage psychosis could result in brain changes and poor disease outcomes. We hypothesized that substantial neuroimaging alterations may exist among patients who experience relapse in early-stage psychosis.
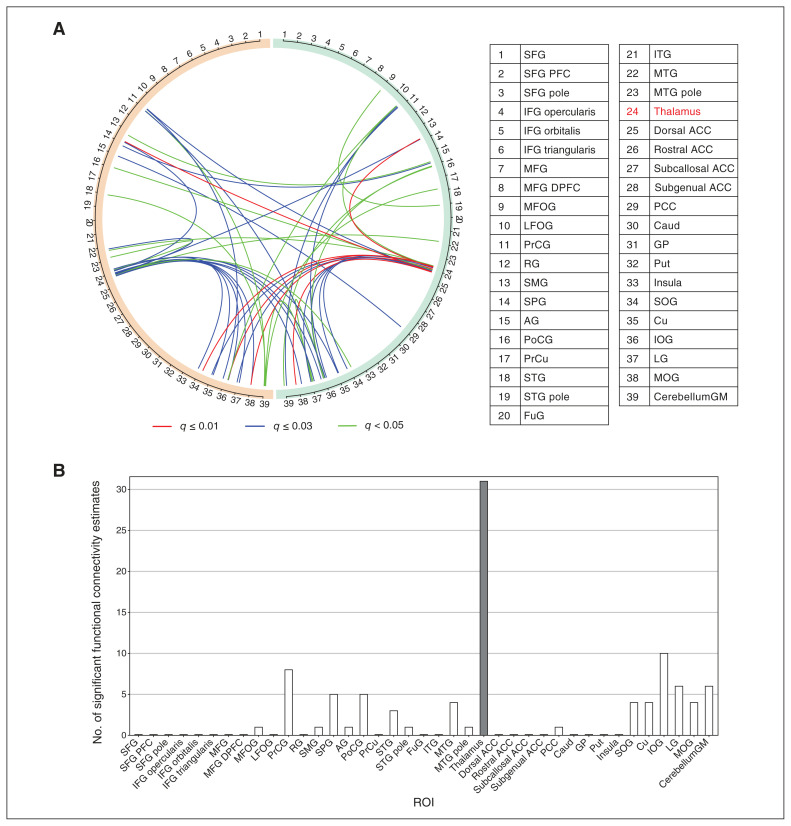
Methods: We studied patients with psychosis within 2 years after the first psychotic event and healthy controls. We divided patients into 2 groups, namely those who did not experience relapse between disease onset and the magnetic resonance imaging (MRI) scan (no-relapse group) and those who did experience relapse between these 2 timings (relapse group). We analyzed 3003 functional connectivity estimates between 78 regions of interest (ROIs) derived from resting-state functional MRI data by adjusting for demographic and clinical confounding factors.
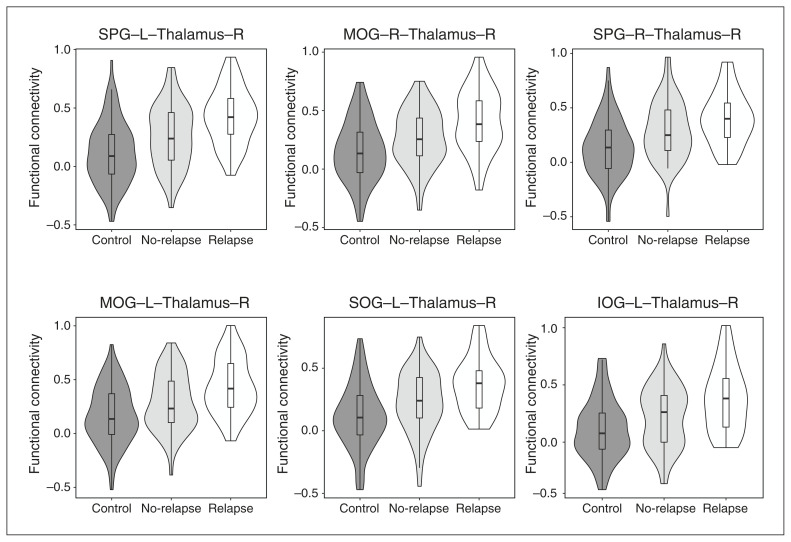
Results: We studied 85 patients, incuding 54 in the relapse group and 31 in the no-relapse group, along with 94 healthy controls. We observed significant differences in 47 functional connectivity estimates between the relapse and control groups after multiple comparison corrections, whereas no differences were found between the no-relapse and control groups. Most of these pathological signatures (64%) involved the thalamus. The Jonckheere-Terpstra test indicated that all 47 functional connectivity changes had a significant cross-group progression from controls to patients in the no-relapse group to patients in the relapse group.
Limitations: Longitudinal studies are needed to further validate the involvement and pathological importance of the thalamus in relapse.
Conclusion: We observed pathological differences in neuronal connectivity associated with relapse in early-stage psychosis, which are more specifically associated with the thalamus. Our study implies the importance of considering neurobiological mechanisms associated with relapse in the trajectory of psychotic disorders.
© 2024 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests:: Frederik Nucifora reports participation on an advisory board with Newron Pharmaceuticals. No other competing interests were declared.
Figures
References
-
- Kahn RS, Sommer IE, Murray RM, et al. . Schizophrenia. Nat Rev Dis Primers 2015;1:15067. - PubMed
-
- Wunderink L, van Bebber J, Sytema S, et al. . Negative symptoms predict high relapse rates and both predict less favorable functional outcome in first episode psychosis, independent of treatment strategy. Schizophr Res 2020;216:192–9. - PubMed
-
- Alvarez-Jimenez M, Priede A, Hetrick SE, et al. . Risk factors for relapse following treatment for first episode psychosis: a systematic review and meta-analysis of longitudinal studies. Schizophr Res 2012;139:116–28. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical