

Progression from ductal carcinoma in situ to invasive breast cancer: molecular features and clinical significance
- PMID: 38570490
- PMCID: PMC10991592
- DOI: 10.1038/s41392-024-01779-3
Progression from ductal carcinoma in situ to invasive breast cancer: molecular features and clinical significance
Abstract
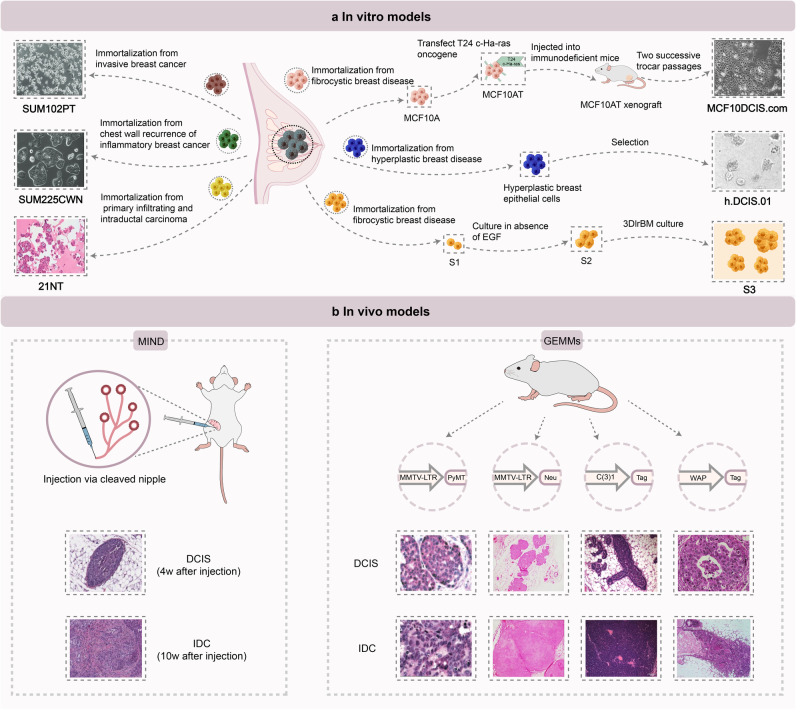
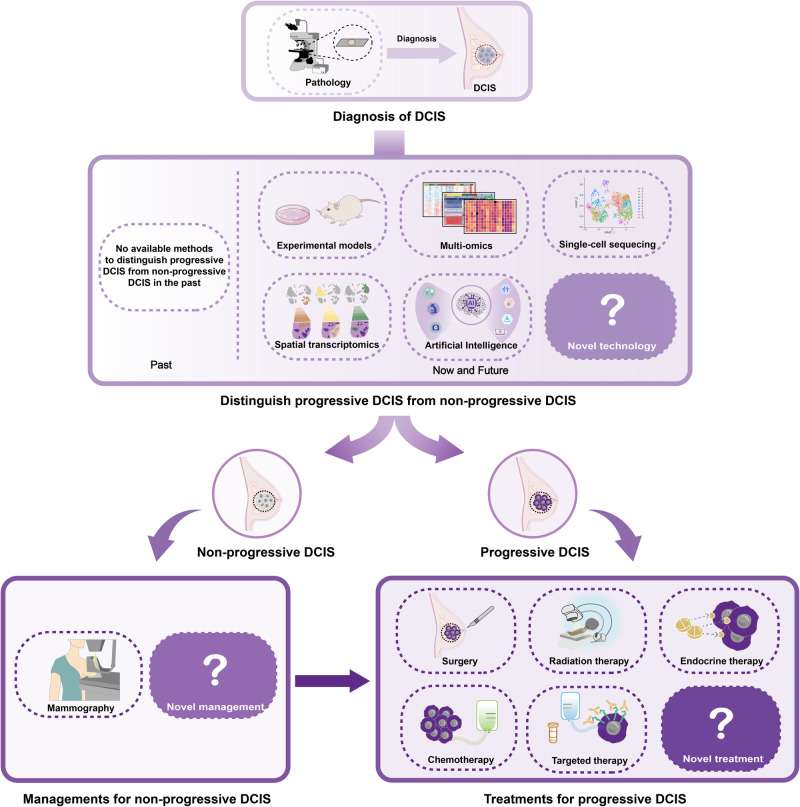
Ductal carcinoma in situ (DCIS) represents pre-invasive breast carcinoma. In untreated cases, 25-60% DCIS progress to invasive ductal carcinoma (IDC). The challenge lies in distinguishing between non-progressive and progressive DCIS, often resulting in over- or under-treatment in many cases. With increasing screen-detected DCIS in these years, the nature of DCIS has aroused worldwide attention. A deeper understanding of the biological nature of DCIS and the molecular journey of the DCIS-IDC transition is crucial for more effective clinical management. Here, we reviewed the key signaling pathways in breast cancer that may contribute to DCIS initiation and progression. We also explored the molecular features of DCIS and IDC, shedding light on the progression of DCIS through both inherent changes within tumor cells and alterations in the tumor microenvironment. In addition, valuable research tools utilized in studying DCIS including preclinical models and newer advanced technologies such as single-cell sequencing, spatial transcriptomics and artificial intelligence, have been systematically summarized. Further, we thoroughly discussed the clinical advancements in DCIS and IDC, including prognostic biomarkers and clinical managements, with the aim of facilitating more personalized treatment strategies in the future. Research on DCIS has already yielded significant insights into breast carcinogenesis and will continue to pave the way for practical clinical applications.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
- 82172344/National Natural Science Foundation of China (National Science Foundation of China)
- LY21H160039/Natural Science Foundation of Zhejiang Province (Zhejiang Provincial Natural Science Foundation)
- LGF21H030010/Natural Science Foundation of Zhejiang Province (Zhejiang Provincial Natural Science Foundation)
LinkOut - more resources
Full Text Sources
Medical
