

Treatment intensification with bempedoic acid to achieve LDL-C goal in patients with ASCVD: A simulation model using a real-world patient cohort in the US
- PMID: 38571880
- PMCID: PMC10987878
- DOI: 10.1016/j.athplu.2024.01.006
Treatment intensification with bempedoic acid to achieve LDL-C goal in patients with ASCVD: A simulation model using a real-world patient cohort in the US
Abstract
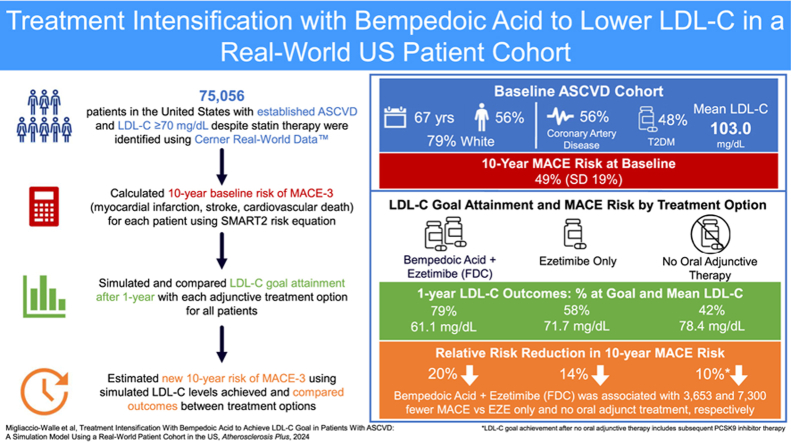
Background and aims: Guidelines recommend that high-risk patients with atherosclerotic cardiovascular disease (ASCVD) be treated with maximally tolerated statins to lower low-density lipoprotein cholesterol (LDL-C) levels and reduce the risk of major adverse cardiovascular events. In patients whose LDL-C remains elevated, non-statin adjunct therapies, including ezetimibe (EZE), bempedoic acid (BA), and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors are recommended.
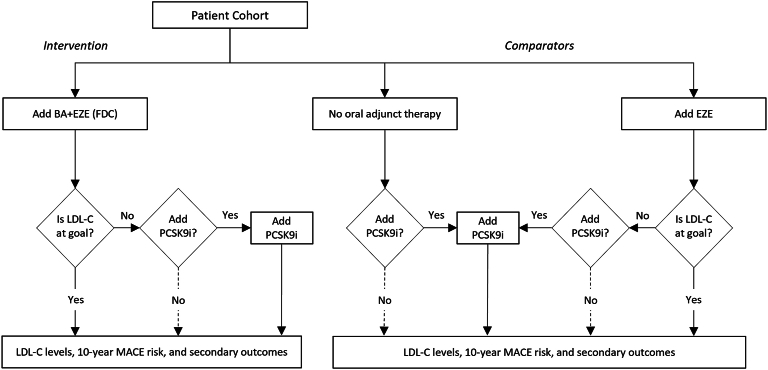
Methods: The impact of BA and EZE in a fixed-dose combination (FDC) on LDL-C goal attainment was evaluated using a simulation model developed for a United States cohort of high-risk adults with ASCVD. Treatment was simulated for 73,056 patients not at goal (LDL-C >70 mg/dL), comparing BA + EZE (FDC), EZE only, and no oral adjunct therapy (NOAT). The addition of PCSK9 inibitors was assumed after 1 year in patients not at LDL-C goal. Treatment efficacy was estimated from clinical trials. Patient-level outcomes were predicted over a 10-year horizon accounting for treatment discontinuation and general mortality.
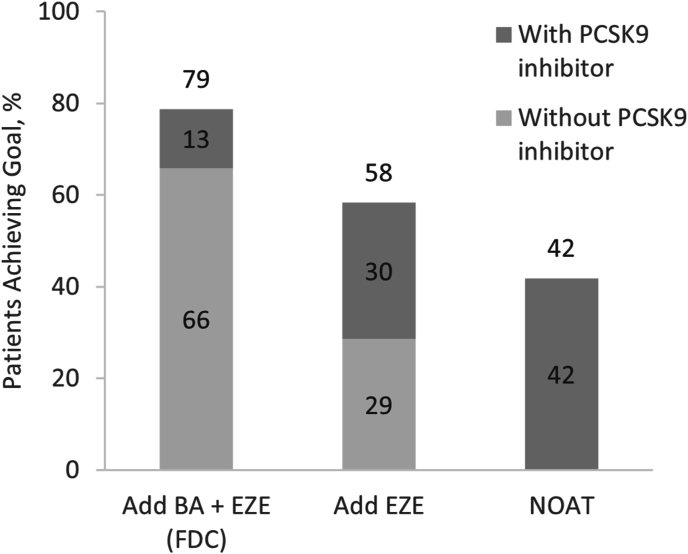
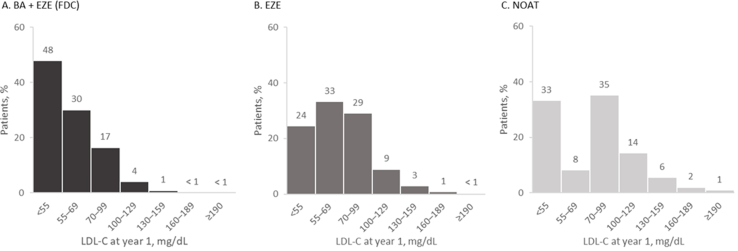
Results: Baseline mean age of the cohort was 67 years, most were White (79%) and male (56%). A majority had established coronary artery disease (75%), 48% had diabetes, and mean LDL-C was 103.0 mg/dL. After 1 year, 79% of patients achieved LDL-C goal (mean, 61.1 mg/dL) with BA + EZE (FDC) compared to 58% and 42% with EZE (71.7 mg/dL) and NOAT (78.4 mg/dL), respectively.
Conclusions: This simulation shows that adding BA + EZE (FDC) to maximally tolerated statins would result in more patients achieving LDL-C goal than adding EZE alone or NOAT.
© 2024 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Kristen Migliaccio-Walle reports financial support was provided by Esperion Therapeutics Inc. Kristen Migliaccio-Walle reports writing assistance was provided by Spark Therapeutics Inc. David Elsea, Kristel Griffith, Rajshree Pandey reports financial support was provided by Esperion Therapeutics Inc. Anand Gupta reports financial support was provided by Esperion Therapeutics Inc. Evelyn Sarnes, Kristin Gillard reports writing assistance was provided by Spark Therapeutics Inc. Evelyn Sarnes, Kristin Gillard reports a relationship with Esperion Therapeutics Inc that includes: employment and equity or stocks. co-author previously employed by Genetech Inc - RP.
Figures
Similar articles
-
Potential Cardiovascular Events Avoided with Bempedoic Acid Plus Ezetimibe Fixed-Dose Combination Compared with Ezetimibe Alone in Patients with Atherosclerotic Cardiovascular Disease Taking Maximally Tolerated Statins.Am J Cardiovasc Drugs. 2023 Jan;23(1):67-76. doi: 10.1007/s40256-022-00552-7. Epub 2022 Oct 31. Am J Cardiovasc Drugs. 2023. PMID: 36316612 Free PMC article. Clinical Trial.
-
Effect of bempedoic acid plus ezetimibe fixed-dose combination vs ezetimibe or placebo on low-density lipoprotein cholesterol in patients with type 2 diabetes and hypercholesterolemia not treated with statins.Am J Prev Cardiol. 2021 Oct 4;8:100278. doi: 10.1016/j.ajpc.2021.100278. eCollection 2021 Dec. Am J Prev Cardiol. 2021. PMID: 34746903 Free PMC article.
-
Simulation of Lipid-Lowering Therapy Intensification in a Population With Atherosclerotic Cardiovascular Disease.JAMA Cardiol. 2017 Sep 1;2(9):959-966. doi: 10.1001/jamacardio.2017.2289. JAMA Cardiol. 2017. PMID: 28768335 Free PMC article.
-
Lipid-lowering treatment up to one year after acute coronary syndrome: guidance from a French expert panel for the implementation of guidelines in practice.Panminerva Med. 2023 Jun;65(2):244-249. doi: 10.23736/S0031-0808.22.04777-2. Epub 2022 Oct 12. Panminerva Med. 2023. PMID: 36222543 Review.
-
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways.J Am Coll Cardiol. 2017 Oct 3;70(14):1785-1822. doi: 10.1016/j.jacc.2017.07.745. Epub 2017 Sep 5. J Am Coll Cardiol. 2017. PMID: 28886926
Cited by
-
New Approaches to Lipoproteins for the Prevention of Cardiovascular Events.J Atheroscler Thromb. 2025 Mar 1;32(3):265-280. doi: 10.5551/jat.RV22031. Epub 2024 Dec 28. J Atheroscler Thromb. 2025. PMID: 39756980 Free PMC article. Review.
References
-
- Grundy S.M., Stone N.J., Bailey A.L., Beam C., Birtcher K.K., et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2018;73:3168–3209. doi: 10.1016/j.jacc.2018.11.002. 2019. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous