

Associated Factors of Cardiopulmonary Resuscitation Outcomes; a Cohort Study on an Adult In-hospital Cardiac Arrest Registry
- PMID: 38572213
- PMCID: PMC10988187
- DOI: 10.22037/aaem.v12i1.2227
Associated Factors of Cardiopulmonary Resuscitation Outcomes; a Cohort Study on an Adult In-hospital Cardiac Arrest Registry
Abstract
Introduction: In-hospital cardiac arrest (IHCA) remains a substantial cause of morbidity and mortality for hospitalized patients worldwide. This study aimed to identify associated factors of return of spontaneous circulation (ROSC) and survival with favorable neurological outcomes of IHCA patients.
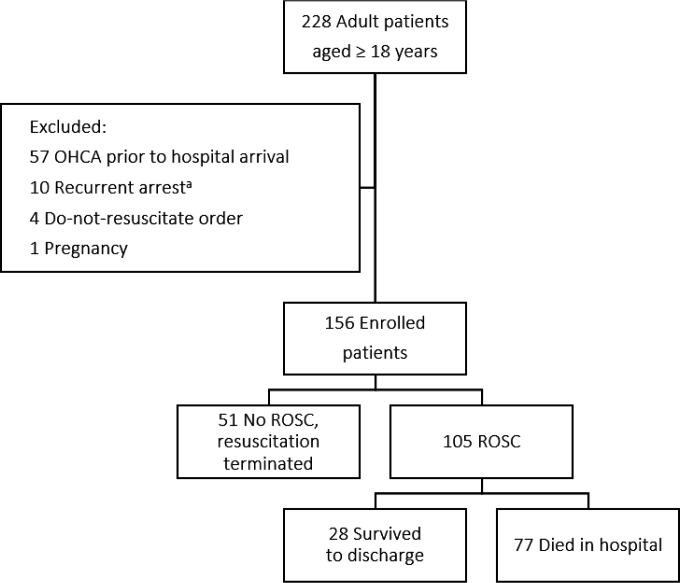
Method: A two-year retrospective cohort study was conducted at a university-based tertiary care hospital in Bangkok, Thailand, studying adult patients aged ≥ 18 years with IHCA from January 2021 to December 2022. The primary endpoint was sustained ROSC, and the secondary endpoint was survival with favorable neurological outcomes defined as Cerebral Performance Categories (CPC) Scale of 1 or 2 at discharge. Pre-arrest and intra-arrest variables were collected and analyzed using multivariable logistic regression to identify independent factors associated with the outcomes.
Results: During the study period, 156 patients were included in the study. 105 (67.3%) patients achieved sustained ROSC after the CPR, 28 patients (18.0%) were discharged alive, and 15 patients (9.6%) survived with a favorable neurological outcome at hospital discharge. Overall, sustained ROSC was higher in patients who had IHCA during the day shift (odds ratio (OR): 4.11; 95% confidence interval (CI): 1.05-16.06) and electrocardiogram (ECG) monitoring prior to arrest (OR: 6.38; 95% CI: 1.18-34.54). In contrast, higher adrenaline doses administrated, and increased CPR duration reduced the odds of sustained ROSC (OR: 0.72; 95% CI: 0.54-0.94 and OR: 0.92; 95% CI: 0.85-0.98, respectively). Arrest due to cardiac etiology was associated with increased discharged survival with favorable neurological outcomes (OR: 13.43; 95% CI: 2.00-89.80), while a higher Good Outcome Following Attempted Resuscitation (GO-FAR) score reduced the odds of the secondary outcome (OR: 0.89; 95% CI: 0.81-0.98).
Conclusion: The sustained ROSC was higher in IHCA during the daytime shift and under prior ECG monitoring. The administration of higher doses of adrenaline and prolonged CPR durations decreased the likelihood of achieving sustained ROSC. Furthermore, patients with cardiac-related causes of cardiac arrest exhibited a higher rate of survival to hospital discharge with favorable neurological outcomes.
Keywords: Heart arrest; Hospitalization; Outcome assessment; Prognosis; Survival; health care.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
[Analysis of the factors influencing prognosis of the adult in-hospital cardiac arrest].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Apr;36(4):398-403. doi: 10.3760/cma.j.cn121430-20230721-00538. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38813635 Chinese.
-
Impact of Early Vasopressor Administration on Neurological Outcomes after Prolonged Out-of-Hospital Cardiac Arrest.Prehosp Disaster Med. 2017 Jun;32(3):297-304. doi: 10.1017/S1049023X17000115. Epub 2017 Feb 22. Prehosp Disaster Med. 2017. PMID: 28222830
-
Associations between red cell distribution width and outcomes of adults with in-hospital cardiac arrest: A retrospective study.Medicine (Baltimore). 2022 Jan 28;101(4):e28750. doi: 10.1097/MD.0000000000028750. Medicine (Baltimore). 2022. PMID: 35089252 Free PMC article.
-
Survival outcome among patients with out-of-hospital cardiac arrest who received cardiopulmonary resuscitation in China: a systematic review and meta-analysis.Eur J Med Res. 2023 Jan 4;28(1):8. doi: 10.1186/s40001-022-00955-x. Eur J Med Res. 2023. PMID: 36600249 Free PMC article.
-
The impact of the SARS-CoV-2 pandemic on in-hospital cardiac arrest: A systematic review and meta-analysis.Resusc Plus. 2024 Sep 4;20:100756. doi: 10.1016/j.resplu.2024.100756. eCollection 2024 Dec. Resusc Plus. 2024. PMID: 39323494 Free PMC article. Review.
Cited by
-
Effects of Emergency Medical Service Response Time on Survival Rate of Out-of-Hospital Cardiac Arrest Patients: a 5-Year Retrospective Study.Arch Acad Emerg Med. 2025 Feb 25;13(1):e36. doi: 10.22037/aaemj.v13i1.2596. eCollection 2025. Arch Acad Emerg Med. 2025. PMID: 40352099 Free PMC article.
-
Performance improvers in cardio-pulmonary resuscitation: a qualitative study.BMC Emerg Med. 2025 Jul 15;25(1):122. doi: 10.1186/s12873-025-01281-1. BMC Emerg Med. 2025. PMID: 40660099 Free PMC article.
-
Point-of-Care Testing (POCT) for Blood Gas and Electrolyte Analysis in Out-of-Hospital Cardiac Arrests' Management; a Cross-sectional Study.Arch Acad Emerg Med. 2025 Jan 25;13(1):e32. doi: 10.22037/aaemj.v13i1.2590. eCollection 2025. Arch Acad Emerg Med. 2025. PMID: 40027219 Free PMC article.
-
A Glance at Archives of Academic Emergency Medicine Journal in 2024.Arch Acad Emerg Med. 2024 Nov 19;13(1):e0. doi: 10.22037/aaem.v13i1.2571. eCollection 2025. Arch Acad Emerg Med. 2024. PMID: 40487906 Free PMC article. No abstract available.
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020;141(9):e139–e596. - PubMed
-
- Schluep M, Gravesteijn BY, Stolker RJ, Endeman H, Hoeks SE. One-year survival after in-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation. 2018;132:90–100. - PubMed
-
- Berg KM, Cheng A, Panchal AR, Topjian AA, Aziz K, Bhanji F, et al. Part 7: Systems of Care: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S580–s604. - PubMed
-
- Nas J, te Grotenhuis R, Bonnes JL, Furlaneto JM, van Royen N, Smeets JLRM, et al. Meta-Analysis Comparing Cardiac Arrest Outcomes Before and After Resuscitation Guideline Updates. The American Journal of Cardiology. 2020;125(4):618–29. - PubMed
LinkOut - more resources
Full Text Sources