

Ionized and total magnesium levels in patients with chronic kidney disease: associated factors and outcomes
- PMID: 38572502
- PMCID: PMC10986257
- DOI: 10.1093/ckj/sfae046
Ionized and total magnesium levels in patients with chronic kidney disease: associated factors and outcomes
Abstract
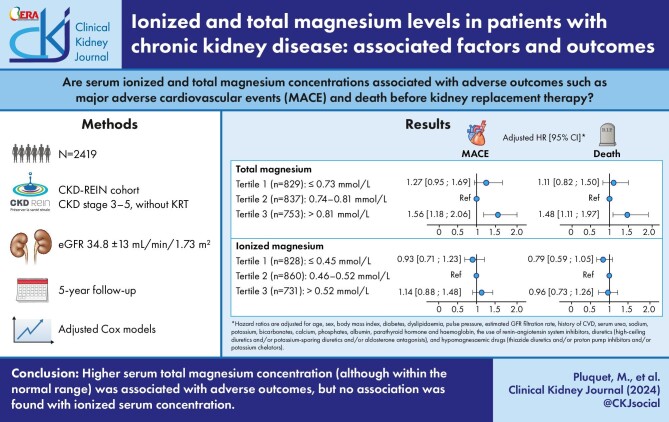
Background: The association between hypo- and/or hypermagnesaemia and cardiovascular (CV) outcomes or mortality has shown conflicting results in chronic kidney disease (CKD) and has been conducted on total magnesium (tMg) levels. Thus, the objectives of the present study were to (i) describe the serum ionized Mg (iMg) concentration in patients at various CKD stages, (ii) measure the correlation between iMg and tMg concentrations, (iii) identify their associated factors and (iv) determine whether serum tMg and/or iMg concentrations are associated with major adverse cardiovascular events (MACE) and mortality before kidney replacement therapy in CKD patients.
Methods: Chronic Kidney Disease-Renal Epidemiology and Information Network (CKD-REIN) is a prospective cohort of CKD patients with an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2. Baseline iMg and tMg serum concentrations were centrally measured. Adjusted cause-specific Cox proportional hazard models were used to estimate hazard ratios (HRs) for first MACE and for mortality.
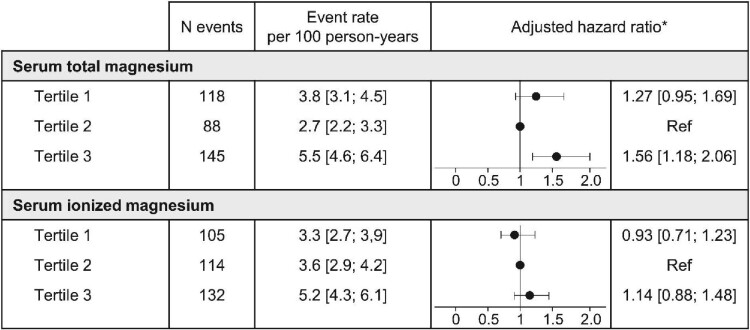
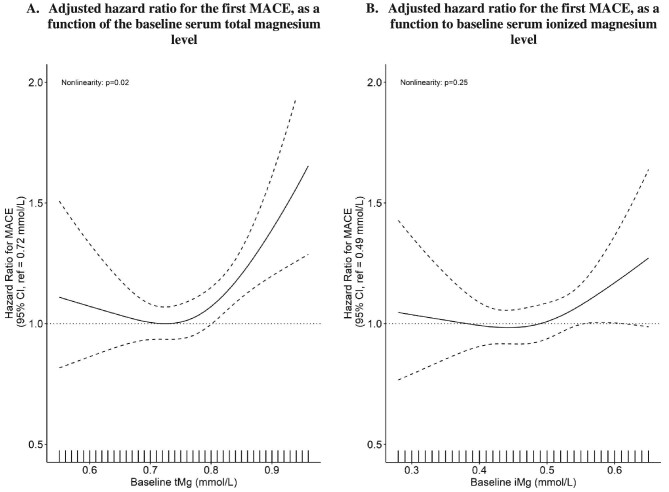
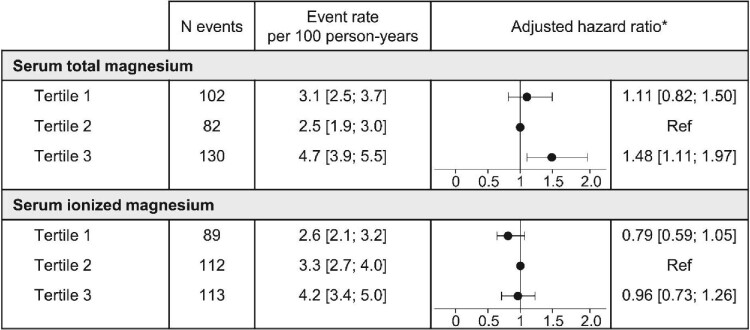
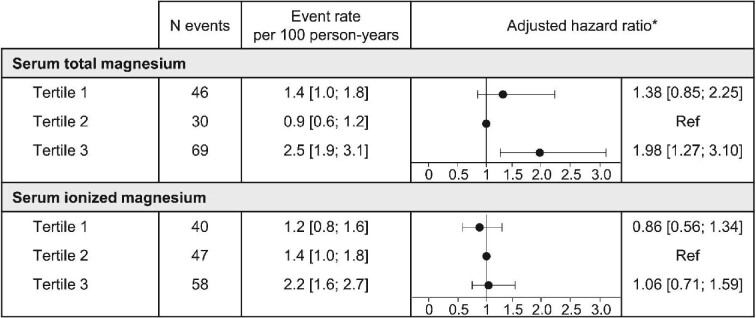
Results: Of the 2419 included patients, median age was 68 years, and the mean eGFR was 34.8 mL/min/1.73 m2. Concentrations of serum iMg and tMg were strongly correlated (r = 0.89, P < .001) and were independently associated with eGFR. The adjusted HR [95% confidence interval (CI)] for MACE associated with the baseline serum tMg level was 1.27 (0.95; 1.69) for patients in Tertile 1 and 1.56 (1.18; 2.06) for patients in Tertile 3, relative to patients in Tertile 2. The HR (95% CI) of death according to serum tMg concentration was increased in Tertile 3 [1.48 (1.11; 1.97)]. The adjusted risk for MACE and mortality (all-cause or CV) associated with the baseline serum iMg level was not significantly different between tertiles.
Conclusions: Our analysis of a large cohort of patients with moderate-to-advanced CKD demonstrated that individuals with higher serum tMg concentrations, although still within the normal range, had a greater likelihood of MACE and mortality. However, serum iMg levels were not associated with these outcomes.
Keywords: cardiovascular disease; chronic kidney disease; magnesium; mortality.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
M.P., S.M.L., S.L., S.K. and M.M. have nothing to declare. Z.A.M. reports having received grants for CKD-REIN and other research projects from Amgen, Baxter, Fresenius Medical Care, GlaxoSmithKline, Merrck Sharp & Dohme-Chibret, Sanofi-Genzyme, Lilly, Otsuka, AstraZeneca, Vifor and the French government, as well as fees and grants to charities from AstraZeneca, Boehringer Ingelheim and GlaxoSmithKline. N.A.P. declare financial support from pharmaceutical companies integrating the public–private partnership of the CKD-REIN cohort: Fresenius Medical Care, GlaxoSmithKline (GSK), Vifor France and Boeringher Ingelheim; all grants are made to Paris Saclay University.
Figures
Similar articles
-
Prevalence, clinical characteristics, and health outcomes of dysmagnesemia measured by ionized and total body concentrations among medically hospitalized patients.Sci Rep. 2024 Oct 10;14(1):23668. doi: 10.1038/s41598-024-74920-5. Sci Rep. 2024. PMID: 39390055 Free PMC article.
-
Homocitrulline is Associated with Cardiovascular Outcomes in Non-Dialysis Patients with CKD.Kidney360. 2025 Apr 1. doi: 10.34067/KID.0000000797. Online ahead of print. Kidney360. 2025. PMID: 40168087
-
Ionized Magnesium Correlates With Total Blood Magnesium in Pediatric Patients Following Kidney Transplant.Ann Lab Med. 2024 Jan 1;44(1):21-28. doi: 10.3343/alm.2024.44.1.21. Epub 2023 Sep 4. Ann Lab Med. 2024. PMID: 37665282 Free PMC article.
-
Systematic Review and Meta-Analysis to Estimate a Reference Range for Circulating Ionized Magnesium Concentrations in Adult Populations.J Nutr. 2023 Dec;153(12):3458-3471. doi: 10.1016/j.tjnut.2023.10.006. Epub 2023 Oct 14. J Nutr. 2023. PMID: 37844840
-
Serum magnesium, mortality, and cardiovascular disease in chronic kidney disease and end-stage renal disease patients: a systematic review and meta-analysis.J Nephrol. 2019 Oct;32(5):791-802. doi: 10.1007/s40620-019-00601-6. Epub 2019 Mar 19. J Nephrol. 2019. PMID: 30888644
Cited by
-
Ionized and total magnesium levels and health outcomes in patients with type 2 diabetes mellitus.Sci Rep. 2025 Feb 5;15(1):4329. doi: 10.1038/s41598-025-88081-6. Sci Rep. 2025. PMID: 39910256 Free PMC article.
-
The importance of measuring the levels of ionized magnesium in the blood in critically ill patients.J Med Biochem. 2025 Jun 13;44(3):386-399. doi: 10.5937/jomb0-54782. J Med Biochem. 2025. PMID: 40821646 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
