

Severity of Respiratory Syncytial Virus vs COVID-19 and Influenza Among Hospitalized US Adults
- PMID: 38573635
- PMCID: PMC11192181
- DOI: 10.1001/jamanetworkopen.2024.4954
Severity of Respiratory Syncytial Virus vs COVID-19 and Influenza Among Hospitalized US Adults
Abstract
Importance: On June 21, 2023, the Centers for Disease Control and Prevention recommended the first respiratory syncytial virus (RSV) vaccines for adults aged 60 years and older using shared clinical decision-making. Understanding the severity of RSV disease in adults can help guide this clinical decision-making.
Objective: To describe disease severity among adults hospitalized with RSV and compare it with the severity of COVID-19 and influenza disease by vaccination status.
Design, setting, and participants: In this cohort study, adults aged 18 years and older admitted to the hospital with acute respiratory illness and laboratory-confirmed RSV, SARS-CoV-2, or influenza infection were prospectively enrolled from 25 hospitals in 20 US states from February 1, 2022, to May 31, 2023. Clinical data during each patient's hospitalization were collected using standardized forms. Data were analyzed from August to October 2023.
Exposures: RSV, SARS-CoV-2, or influenza infection.
Main outcomes and measures: Using multivariable logistic regression, severity of RSV disease was compared with COVID-19 and influenza severity, by COVID-19 and influenza vaccination status, for a range of clinical outcomes, including the composite of invasive mechanical ventilation (IMV) and in-hospital death.
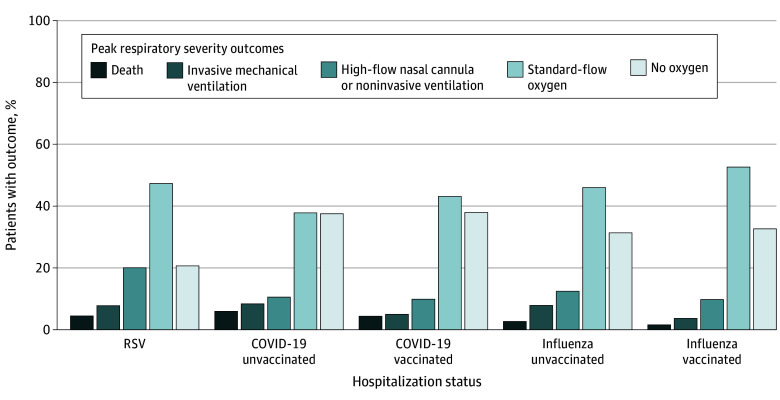
Results: Of 7998 adults (median [IQR] age, 67 [54-78] years; 4047 [50.6%] female) included, 484 (6.1%) were hospitalized with RSV, 6422 (80.3%) were hospitalized with COVID-19, and 1092 (13.7%) were hospitalized with influenza. Among patients with RSV, 58 (12.0%) experienced IMV or death, compared with 201 of 1422 unvaccinated patients with COVID-19 (14.1%) and 458 of 5000 vaccinated patients with COVID-19 (9.2%), as well as 72 of 699 unvaccinated patients with influenza (10.3%) and 20 of 393 vaccinated patients with influenza (5.1%). In adjusted analyses, the odds of IMV or in-hospital death were not significantly different among patients hospitalized with RSV and unvaccinated patients hospitalized with COVID-19 (adjusted odds ratio [aOR], 0.82; 95% CI, 0.59-1.13; P = .22) or influenza (aOR, 1.20; 95% CI, 0.82-1.76; P = .35); however, the odds of IMV or death were significantly higher among patients hospitalized with RSV compared with vaccinated patients hospitalized with COVID-19 (aOR, 1.38; 95% CI, 1.02-1.86; P = .03) or influenza disease (aOR, 2.81; 95% CI, 1.62-4.86; P < .001).
Conclusions and relevance: Among adults hospitalized in this US cohort during the 16 months before the first RSV vaccine recommendations, RSV disease was less common but similar in severity compared with COVID-19 or influenza disease among unvaccinated patients and more severe than COVID-19 or influenza disease among vaccinated patients for the most serious outcomes of IMV or death.
Conflict of interest statement
Figures
References
-
- Melgar M. Evidence to recommendation framework: respiratory syncytial virus (RSV) in adults Presented at the Advisory Committee on Immunization Practices meeting. Atlanta, GA; February 23, 2023. Access on August 7, 2023. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-02/slid...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
