

FOLFIRI Plus Durvalumab With or Without Tremelimumab in Second-Line Treatment of Advanced Gastric or Gastroesophageal Junction Adenocarcinoma: The PRODIGE 59-FFCD 1707-DURIGAST Randomized Clinical Trial
- PMID: 38573643
- PMCID: PMC11190792
- DOI: 10.1001/jamaoncol.2024.0207
FOLFIRI Plus Durvalumab With or Without Tremelimumab in Second-Line Treatment of Advanced Gastric or Gastroesophageal Junction Adenocarcinoma: The PRODIGE 59-FFCD 1707-DURIGAST Randomized Clinical Trial
Abstract
Importance: Efficacy of second-line chemotherapy in advanced gastric or gastrooesphageal junction (GEJ) adenocarcinoma remains limited.
Ojectives: To determine the efficacy of 1 or 2 immune checkpoint inhibitors combined with FOLFIRI (leucovorin [folinic acid], fluorouracil, and irinotecan) in the treatment of advanced gastric/GEJ adenocarcinoma.
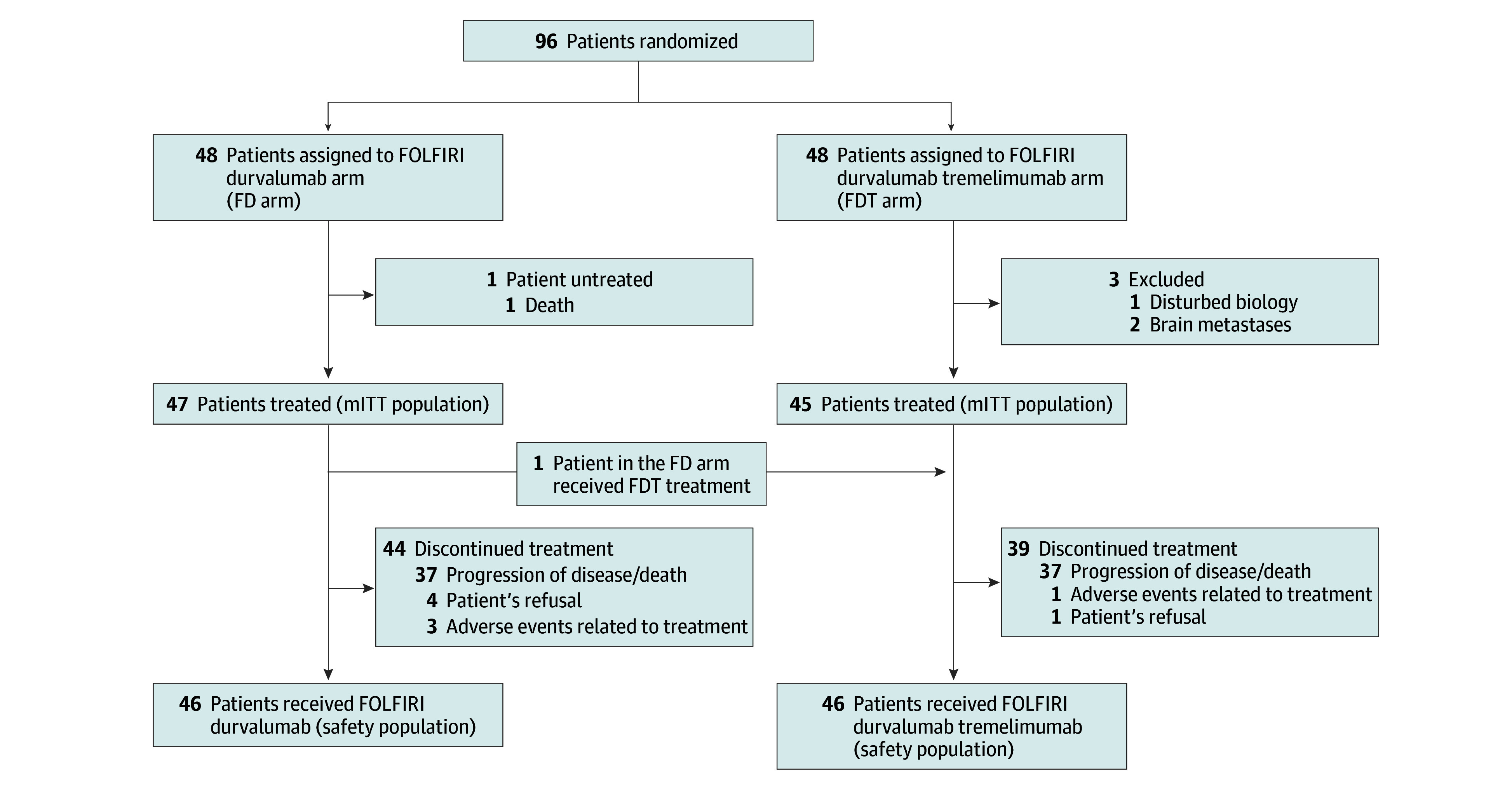
Design, setting, and participants: The PRODIGE 59-FFCD 1707-DURIGAST trial is a randomized, multicenter, noncomparative, phase 2 trial, conducted from August 27, 2020, and June 4, 2021, at 37 centers in France that included patients with advanced gastric/GEJ adenocarcinoma who had disease progression after platinum-based first-line chemotherapy.
Intervention: Patients were randomized to receive FOLFIRI plus durvalumab (anti-programmed cell death 1 [PD-L1]) (FD arm) or FOLFIRI plus durvalumab and tremelimumab (anti-cytotoxic T-lymphocyte associated protein 4 [CTLA-4]) (FDT arm). The efficacy analyses used a clinical cutoff date of January 9, 2023.
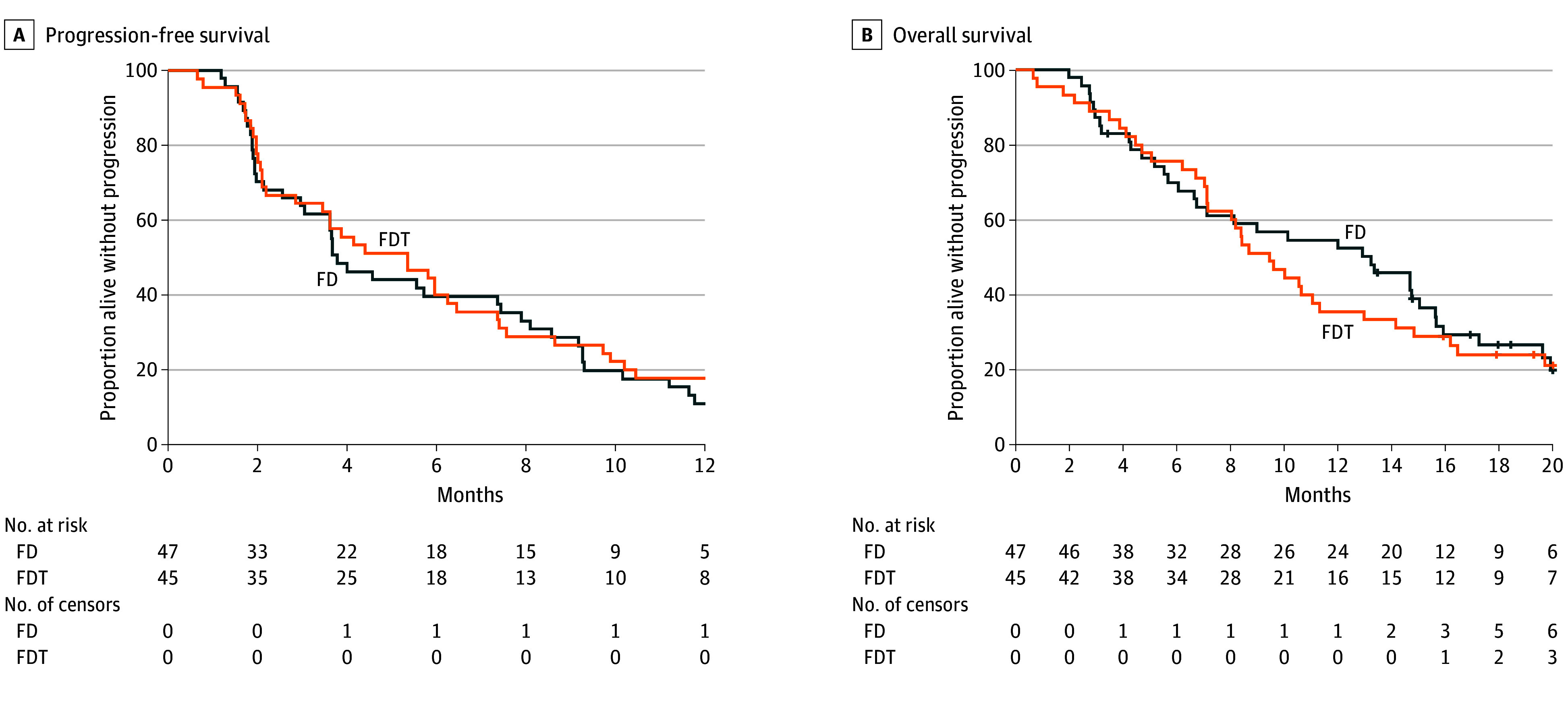
Main outcome and measures: The primary end point was progression-free survival (PFS) at 4 months according to RECIST 1.1 criteria evaluated by investigators.
Results: Overall, between August 27, 2020, and June 4, 2021, 96 patients were randomized (48 in each arm). The median age was 59.7 years, 28 patients (30.4%) were women and 49 (53.3%) had GEJ tumors. Four month PFS was 44.7% (90% CI, 32.3-57.7) and 55.6% (90% CI, 42.3-68.3) in the FD and FDT arms, respectively. The primary end point was not met. Median PFS was 3.8 and 5.4 months, objective response rates were 34.7% and 37.7%, and median overall survival was 13.2 and 9.5 months in the FD and FDT arms, respectively. Disease control beyond 1 year was 14.9% in the FD arm and 24.4% in the FDT arm. Grade 3 to 4 treatment-related adverse events were observed in 22 (47.8%) patients in each arm. A combined positive score (CPS) PD-L1 of 5 or higher was observed in 18 tumors (34.0%) and a tumor proportion score (TPS) PD-L1 of 1% or higher in 13 tumors (24.5%). Median PFS according to CPS PD-L1 was similar (3.6 months for PD-L1 CPS ≥5 vs 5.4 months for PD-L1 CPS <5) by contrast for TPS PD-L1 (6.0 months for PD-L1 TPS ≥1% vs 3.8 months for PD-L1 TPS <1%).
Conclusions and relevance: Combination of immune checkpoint inhibitors with FOLFIRI in second-line treatment for advanced gastric/GEJ adenocarcinoma showed an acceptable safety profile but antitumor activity only in a subgroup of patients.
Trial registration: ClinicalTrials.gov Identifier: NCT03959293.
Conflict of interest statement
Figures
Comment on
-
Immunotherapy in Gastric Cancer-Choosing Methods or Results.JAMA Oncol. 2024 Jun 1;10(6):704-705. doi: 10.1001/jamaoncol.2023.7262. JAMA Oncol. 2024. PMID: 38573642 No abstract available.
References
-
- Van Cutsem E, Moiseyenko VM, Tjulandin S, et al. ; V325 Study Group . Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: a report of the V325 Study Group. J Clin Oncol. 2006;24(31):4991-4997. doi:10.1200/JCO.2006.06.8429 - DOI - PubMed
-
- Al-Batran SE, Hartmann JT, Hofheinz R, et al. . Biweekly fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) for patients with metastatic adenocarcinoma of the stomach or esophagogastric junction: a phase II trial of the Arbeitsgemeinschaft Internistische Onkologie. Ann Oncol. 2008;19(11):1882-1887. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
