

Inflammatory and tissue injury marker dynamics in pediatric acute respiratory distress syndrome
- PMID: 38573766
- PMCID: PMC11093602
- DOI: 10.1172/JCI177896
Inflammatory and tissue injury marker dynamics in pediatric acute respiratory distress syndrome
Abstract
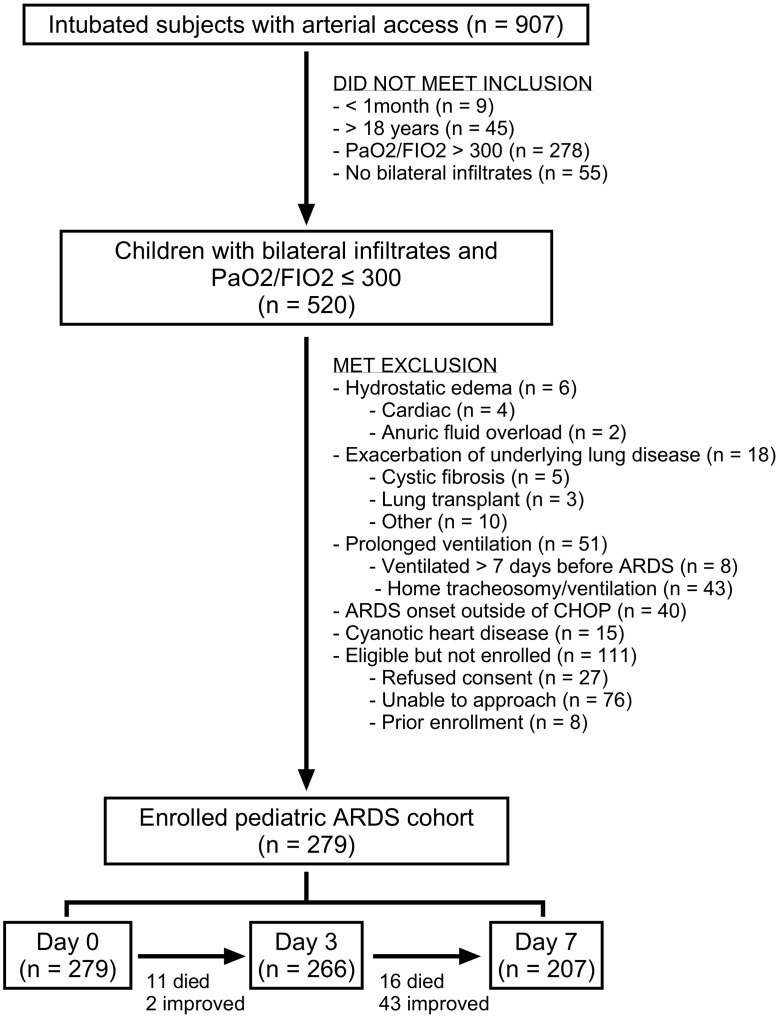
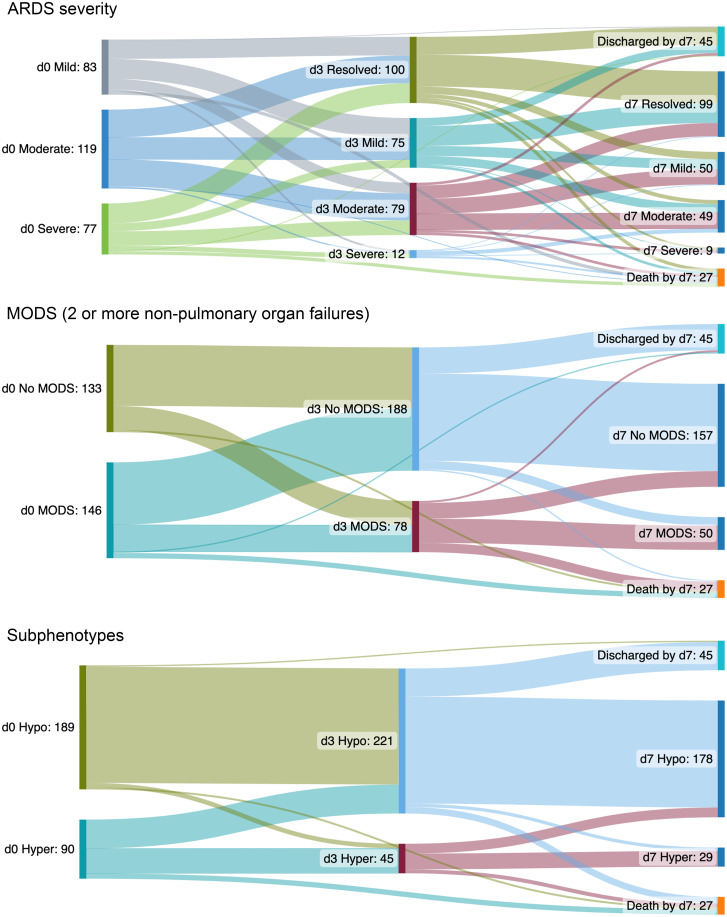
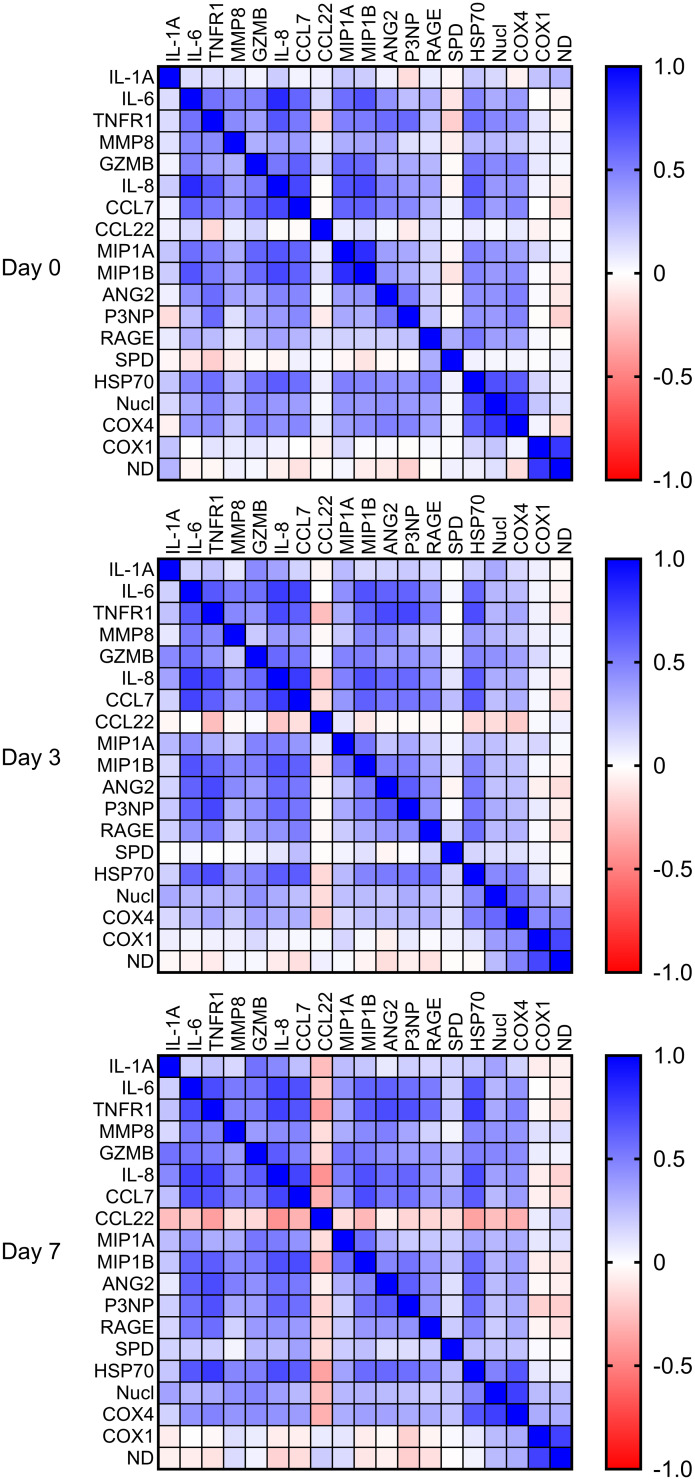
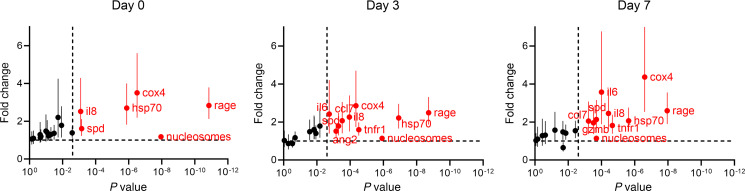
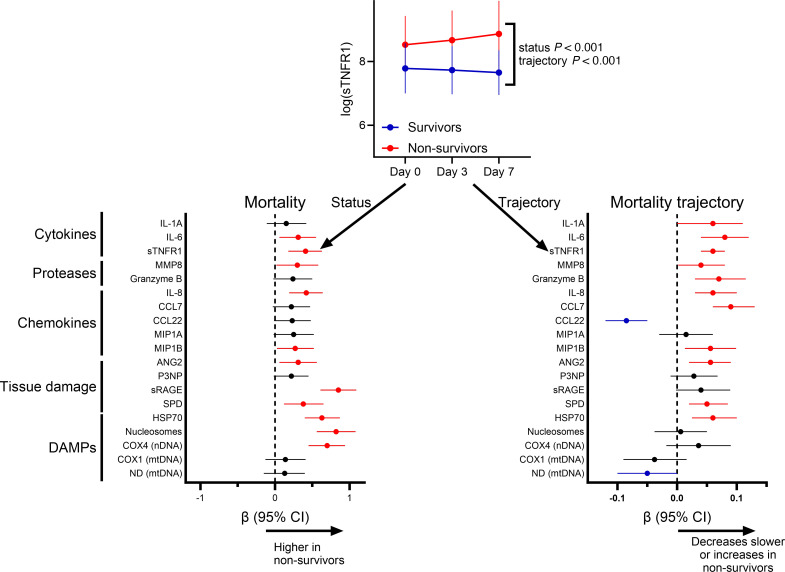
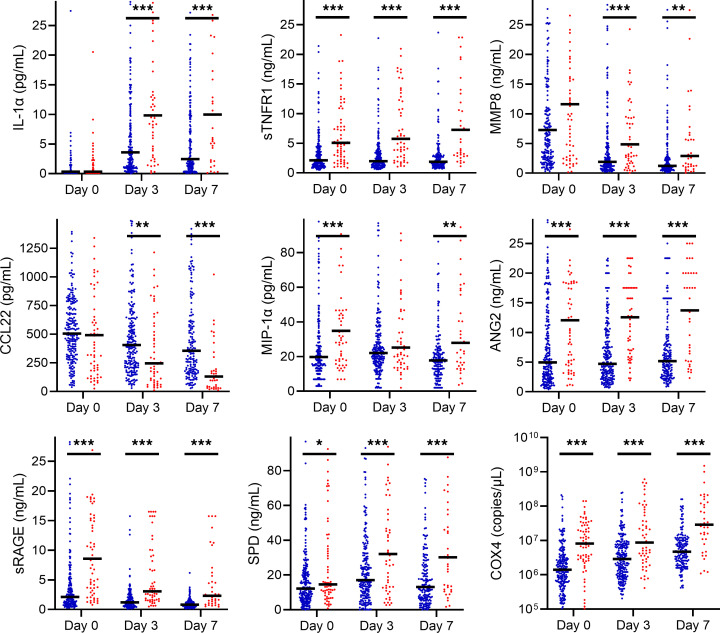
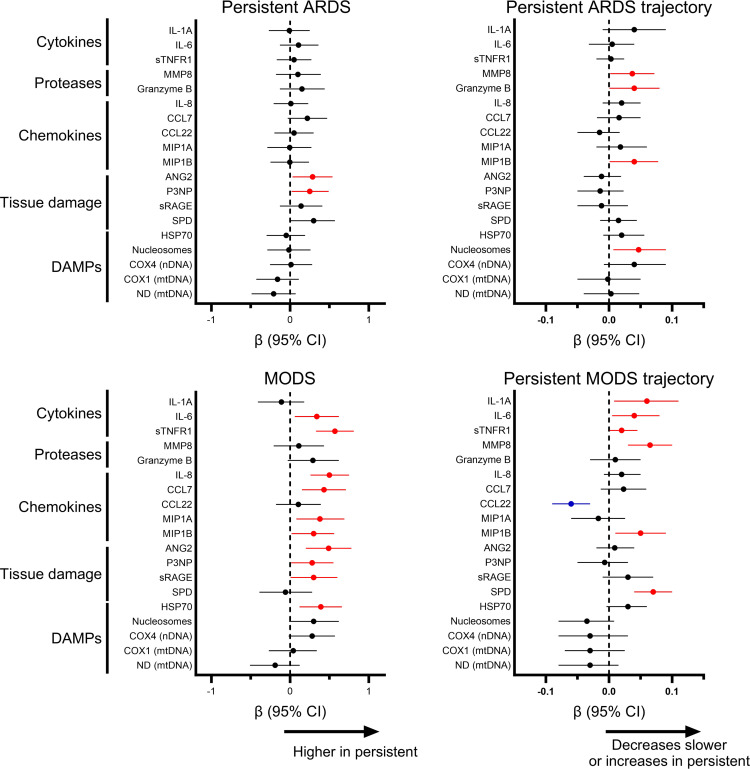
BACKGROUNDThe molecular signature of pediatric acute respiratory distress syndrome (ARDS) is poorly described, and the degree to which hyperinflammation or specific tissue injury contributes to outcomes is unknown. Therefore, we profiled inflammation and tissue injury dynamics over the first 7 days of ARDS, and associated specific biomarkers with mortality, persistent ARDS, and persistent multiple organ dysfunction syndrome (MODS).METHODSIn a single-center prospective cohort of intubated pediatric patients with ARDS, we collected plasma on days 0, 3, and 7. Nineteen biomarkers reflecting inflammation, tissue injury, and damage-associated molecular patterns (DAMPs) were measured. We assessed the relationship between biomarkers and trajectories with mortality, persistent ARDS, or persistent MODS using multivariable mixed effect models.RESULTSIn 279 patients (64 [23%] nonsurvivors), hyperinflammatory cytokines, tissue injury markers, and DAMPs were higher in nonsurvivors. Survivors and nonsurvivors showed different biomarker trajectories. IL-1α, soluble tumor necrosis factor receptor 1, angiopoietin 2 (ANG2), and surfactant protein D increased in nonsurvivors, while DAMPs remained persistently elevated. ANG2 and procollagen type III N-terminal peptide were associated with persistent ARDS, whereas multiple cytokines, tissue injury markers, and DAMPs were associated with persistent MODS. Corticosteroid use did not impact the association of biomarker levels or trajectory with mortality.CONCLUSIONSPediatric ARDS survivors and nonsurvivors had distinct biomarker trajectories, with cytokines, endothelial and alveolar epithelial injury, and DAMPs elevated in nonsurvivors. Mortality markers overlapped with markers associated with persistent MODS, rather than persistent ARDS.FUNDINGNIH (K23HL-136688, R01-HL148054).
Keywords: Endothelial cells; Inflammation; Innate immunity; Proteomics; Pulmonology.
Conflict of interest statement
Figures
Comment in
- Time to split: Biomarker trajectories in pediatric acute respiratory distress syndrome hint at underlying disease
References
-
- Khemani RG, et al. Pediatric acute respiratory distress syndrome: definition, incidence, and epidemiology: proceedings from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med. 2015;16(5 Suppl 1):23–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
