

High risk of lung cancer in surfactant-related gene variant carriers
- PMID: 38575158
- PMCID: PMC11063619
- DOI: 10.1183/13993003.01809-2023
High risk of lung cancer in surfactant-related gene variant carriers
Abstract
Background: Several rare surfactant-related gene (SRG) variants associated with interstitial lung disease are suspected to be associated with lung cancer, but data are missing. We aimed to study the epidemiology and phenotype of lung cancer in an international cohort of SRG variant carriers.
Methods: We conducted a cross-sectional study of all adults with SRG variants in the OrphaLung network and compared lung cancer risk with telomere-related gene (TRG) variant carriers.
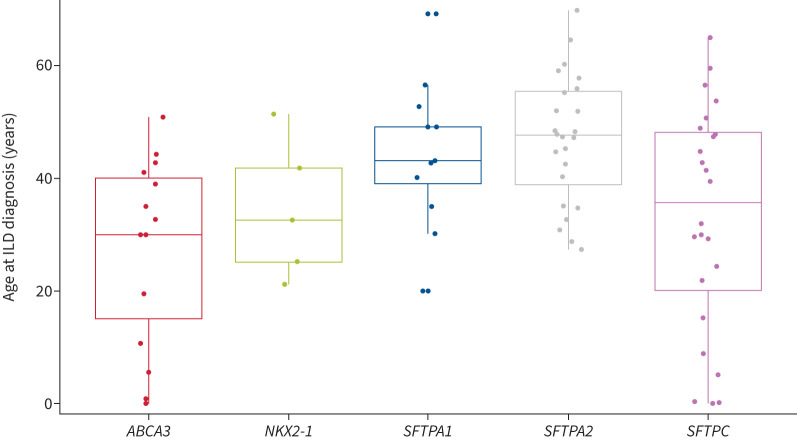
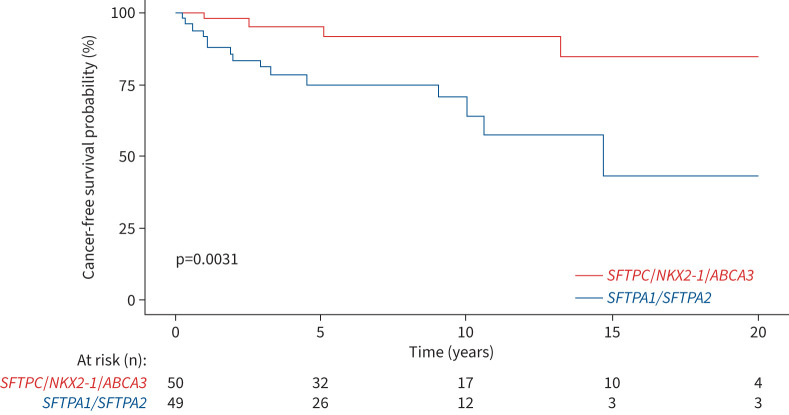
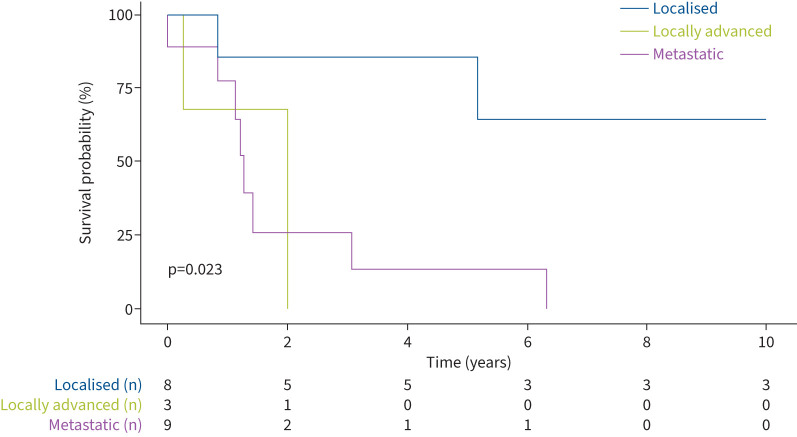
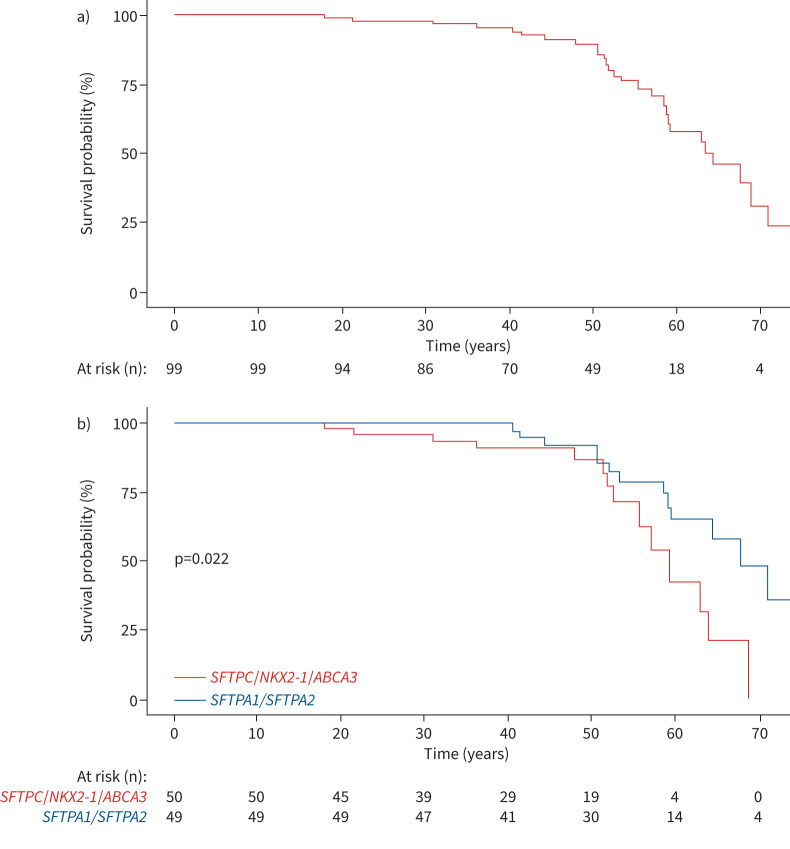
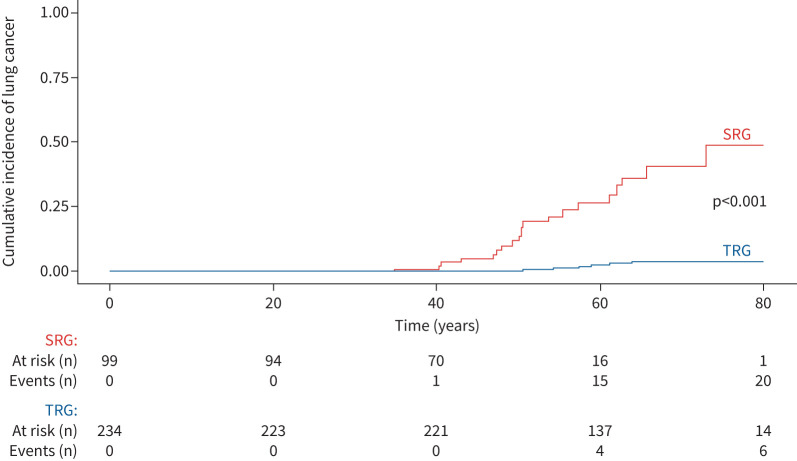
Results: We identified 99 SRG adult variant carriers (SFTPA1 (n=18), SFTPA2 (n=31), SFTPC (n=24), ABCA3 (n=14) and NKX2-1 (n=12)), including 20 (20.2%) with lung cancer (SFTPA1 (n=7), SFTPA2 (n=8), SFTPC (n=3), NKX2-1 (n=2) and ABCA3 (n=0)). Among SRG variant carriers, the odds of lung cancer was associated with age (OR 1.04, 95% CI 1.01-1.08), smoking (OR 20.7, 95% CI 6.60-76.2) and SFTPA1/SFTPA2 variants (OR 3.97, 95% CI 1.39-13.2). Adenocarcinoma was the only histological type reported, with programmed death ligand-1 expression ≥1% in tumour cells in three samples. Cancer staging was localised (I/II) in eight (40%) individuals, locally advanced (III) in two (10%) and metastatic (IV) in 10 (50%). We found no somatic variant eligible for targeted therapy. Seven cancers were surgically removed, 10 received systemic therapy, and three received the best supportive care according to their stage and performance status. The median overall survival was 24 months, with stage I/II cancers showing better survival. We identified 233 TRG variant carriers. The comparative risk (subdistribution hazard ratio) for lung cancer in SRG patients versus TRG patients was 18.1 (95% CI 7.1-44.7).
Conclusions: The high risk of lung cancer among SRG variant carriers suggests specific screening and diagnostic and therapeutic challenges. The benefit of regular computed tomography scan follow-up should be evaluated.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: P. Bonniaud reports grants from AstraZeneca, lecture honoraria from Sanofi and AstraZeneca, travel support from AstraZeneca, Novartis, Sanofi, Boehringer and Stallergenes, and advisory board membership with AstraZeneca, Novartis, Sanofi, GSK and Boehringer. J. Cadranel had a patent planned, received consulting fees and participated on a data safety monitoring board or advisory board for AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, BMS, Daichi, Lilly, Pfizer, Novartis, MSD, Roche and Takeda. A. Cazes reports lecture honoraria and travel support from Boehringer Ingelheim. B. Crestani reports grants from Boehringer Ingelheim, consulting fees from Apellis, BMS, Boehringer Ingelheim and Sanofi, lecture honoraria from Apellis, AstraZeneca, BMS, Boehringer Ingelheim, Novartis and Sanofi, support for attending meetings or travel from AstraZeneca, BMS, Boehringer Ingelheim and Sanofi, participated on a data safety monitoring board or advisory board for Apellis, BMS, Boehringer Ingelheim and Sanofi, and had a leadership role as President of the Board of Trustees of the Fondation du Souffle. R. Epaud reports consulting fees from AstraZeneca, lecture honoraria from GSK, AstraZeneca and Menarini, travel support from GSK and AstraZeneca, and advisory board membership with AstraZeneca and Novartis. M-P. Debray reports lecture honoraria and travel support from Boehringer Ingelheim. E. Manali reports lecture honoraria from Boehringer Ingelheim, CLS Behring and Hoffman-La Roche, support for attending meetings or travel from Boehringer Ingelheim, CLS Behring, Hoffman-La Roche and Elpen, and had a leadership role as a Chair in the ERS Task Force for transition of chILD to adult care. S. Papiris reports lecture honoraria from Boehringer Ingelheim and Hoffmann-La Roche, and travel support from Boehringer Ingelheim and Elpen. N. Nathan reports grants from Legs poix de la Chancellerie des Universités 2022 (number 2022000594). C. Andréjak participated on a data safety monitoring board or advisory board for the EVER-ILD2 study (rituximab in diffuse interstitial pneumonia) and received funding via a grant from the French Research Ministry. S. Jouneau reports grants from AIRB, Boehringer Ingelheim and Roche, lecture honoraria from AIRB, AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Chiesi, Genzyme, GSK, LVL, Novartis, Pfizer, Roche and Sanofi, travel support from Boehringer Ingelheim, Roche and AIRB, and advisory board participation for Boehringer Ingelheim, GSK and Sanofi. G. Beltramo reports lecture honoraria from Bristol Myers Squibb, and support for attending meetings or travel from Sanofi Aventis France and Boehringer Ingelheim France. S. Hirschi reports research grants from Agence de la Biomedécine, CSL Behring and Adiral medical assistance, lecture honoraria from Boehringer Ingelheim, travel support from CSL Behring, Boehringer Ingelheim and ISIS Medical, and received medical equipment from ISIS Medical. C. Picard reports lecture honoraria and consulting fees from Boehringer Ingelheim. G. Prévot reports honoraria for presentations and educational event from Boehringer Ingelheim, Sanofi, Jansen and MSD. G. Zalcman reports consulting fees from AstraZeneca, BMS, Pfizer and Sanofi, lecture honoraria from BMS, AstraZeneca and Sanofi, support for attending meetings or travel from AstraZeneca and BMS, and participated on a data safety monitoring board or advisory board for AstraZeneca and BMS. V. Cottin reports grants from Boehringer Ingelheim, consulting fees from AstraZeneca, Boehringer Ingelheim, Celgene/BMS, CSL Behring, Ferrer/United Therapeutics, GSK, Pliant, Pure Tech, RedX, Roche, Sanofi and Shionogi, lecture honoraria from Boehringer Ingelheim, Ferrer/United Therapeutics and Roche, support for attending meetings or travel from Boehringer Ingelheim and Roche, participated on a data safety monitoring board or advisory board for Galapagos, Galecto and GSK, and had a leadership role in an adjudication committee for Fibrogen. R. Borie reports consulting fees from Boehringer Ingelheim, Ferrer and Sanofi, lecture honoraria from Boehringer Ingelheim and Roche, travel support from Boehringer Ingelheim, Roche and Chiesi, and advisory board participation for Savara. The remaining authors have no potential conflicts of interest to disclose.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous