

The importance of LDL-C lowering in atherosclerotic cardiovascular disease prevention: Lower for longer is better
- PMID: 38576462
- PMCID: PMC10992711
- DOI: 10.1016/j.ajpc.2024.100649
The importance of LDL-C lowering in atherosclerotic cardiovascular disease prevention: Lower for longer is better
Abstract
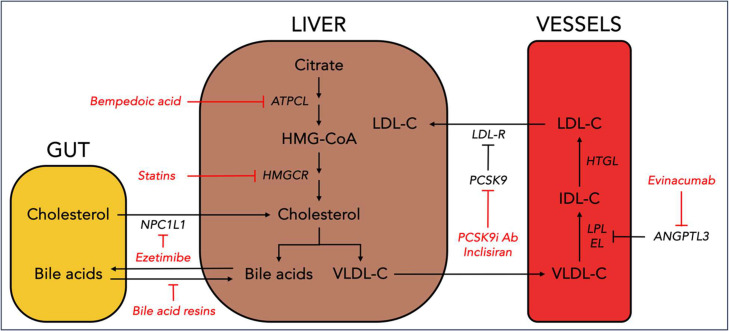
Cumulative exposure to low-density lipoprotein cholesterol (LDL-C) is a key driver of atherosclerotic cardiovascular disease (ASCVD) risk. An armamentarium of therapies to achieve robust and sustained reduction in LDL-C can reduce ASCVD risk. The gold standard for LDL-C assessment is ultracentrifugation but in routine clinical practice LDL-C is usually calculated and the most accurate calculation is the Martin/Hopkins equation. For primary prevention, consideration of estimated ASCVD risk frames decision making regarding use of statins and other therapies, and tools such as risk enhancing factors and coronary artery calcium enable tailoring of risk assessment and decision making. In patients with diabetes, lipid lowering therapy is recommended in most patients to reduce ASCVD risk with an opportunity to tailor therapy based on other risk factors. Patients with primary hypercholesterolemia and familial hypercholesterolemia (FH) with baseline LDL-C greater than or equal to 190 mg/dL are at elevated risk, and LDL-C lowering with high-intensity statin therapy is often combined with non-statin therapies to prevent ASCVD. Secondary prevention of ASCVD, including in patients with prior myocardial infarction or stroke, requires intensive lipid lowering therapy and lifestyle modification approaches. There is no established LDL-C level below which benefit ceases or safety concerns arise. When further LDL-C lowering is required beyond lifestyle modifications and statin therapy, additional medications include oral ezetimibe and bempedoic acid, or injectables such as PCSK9 monoclonal antibodies or siRNA therapy. A novel agent that acts independently of hepatic LDL receptors is evinacumab, which is approved for patients with homozygous FH. Other emerging agents are targeted at Lp(a) and CETP. In light of the expanding lipid treatment landscape, this manuscript reviews the importance of early, intensive, and sustained LDL-C-lowering for primary and secondary prevention of ASCVD.
Keywords: Atherosclerotic cardiovascular disease; LDL cholesterol; Lipid lowering; Non-statin; Primary prevention; Secondary prevention; Statins.
© 2024 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: OM, ZAB, and SLS have no disclosures to report. PK: Speaker's Bureau: Boston Scientific, Amarin, Esperion, AstraZeneca, Merck, Advisory Board: Amgen, Boston Scientific, Novartis, Esperion, Doximity, DocWire/MashUP MD, Honoraria: ACC/ABIM Question Writing, Current Atherosclerosis Reports Section Editor, Amgen, Consultant: Grand Rounds, American College of Cardiology, Grand Rounds, 2nd MD, Writing/Editorial Board: Healthline, GE/SkyWord, American College of Cardiology. Under a license agreement between Corrie Health and Johns Hopkins University, the university owns equity in Corrie Health. The university, FAM and SSM are entitled to royalty distributions related to Corrie Health. In addition, FAM and SSM are co-founders of and hold equity in Corrie Health. This arrangement has been reviewed and approved by Johns Hopkins University in accordance with its conflict of interest policies. FAM and SSM have also received research and material support from Apple and iHealth. Furthermore, SSM is on the Advisory Board for Care Access and reports personal consulting fees from Amgen, AstraZeneca, BMS, Chroma, Kaneka, NewAmsterdam, Novartis, Novo Nordisk, Premier, Sanofi, and 89bio. Outside this work, SSM reports research support from the American Heart Association (20SFRN35380046, 20SFRN35490003, #878,924, #882,415, #946,222), the Patient-Centered Outcomes Research Institute (ME-2019C1–15 328, IHS-2021C3–24,147), the National Institutes of Health (NIH) (P01 HL108800 and R01AG071032), the David and June Trone Family Foundation, the Pollen Digital Innovation Fund, Sandra and Larry Small, Google, and Merck.
Figures
References
-
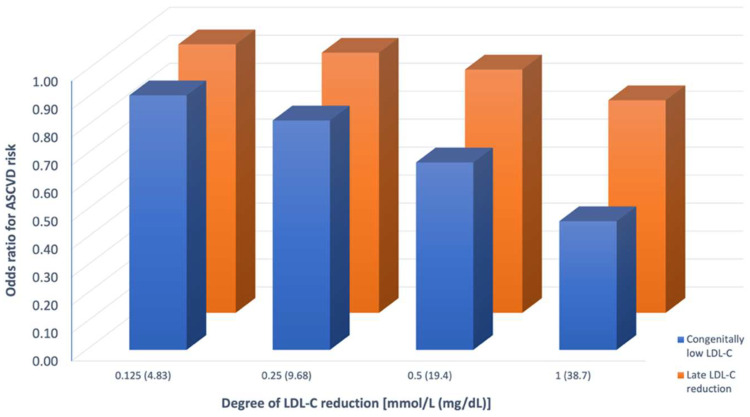
- Ference B.A., Yoo W., Alesh I., et al. Effect of long-term exposure to lower low-density lipoprotein cholesterol beginning early in life on the risk of coronary heart disease: a Mendelian randomization analysis. J Am Coll Cardiol. 2012;60(25):2631–2639. - PubMed
-
- Ference B.A., Ginsberg H.N., Graham I., et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–2472. - PMC - PubMed
-
- Skalen K., Gustafsson M., Rydberg E.K., et al. Subendothelial retention of atherogenic lipoproteins in early atherosclerosis. Nature. 2002;417(6890):750–754. - PubMed
-
- Tabas I., Williams K.J., Boren J. Subendothelial lipoprotein retention as the initiating process in atherosclerosis: update and therapeutic implications. Circulation. 2007;116(16):1832–1844. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
