

Immunovirological status in people with perinatal and adult-acquired HIV-1 infection: a multi-cohort analysis from France
- PMID: 38576825
- PMCID: PMC10993179
- DOI: 10.1016/j.lanepe.2024.100885
Immunovirological status in people with perinatal and adult-acquired HIV-1 infection: a multi-cohort analysis from France
Abstract
Background: No study has compared the virological and immunological status of young people with perinatally-acquired HIV infection (P-HIV) with that of people with HIV adulthood (A-HIV) having a similar duration of infection.
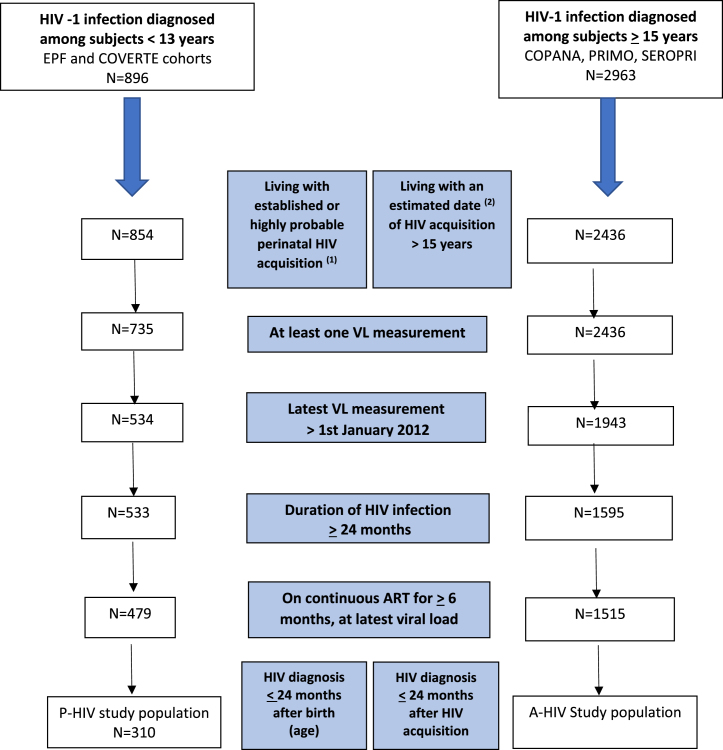
Methods: 5 French cohorts of P-HIV and A-HIV patients with a known date of HIV-infection and receiving antiretroviral treatment (ART), were used to compare the following proportions of: virological failure (VF) defined as plasma HIV RNA ≥ 50 copies/mL, CD4 cell percentages and CD4:CD8 ratios, at the time of the most recent visit since 2012. The analysis was stratified on time since infection, and multivariate models were adjusted for demographics and treatment history.
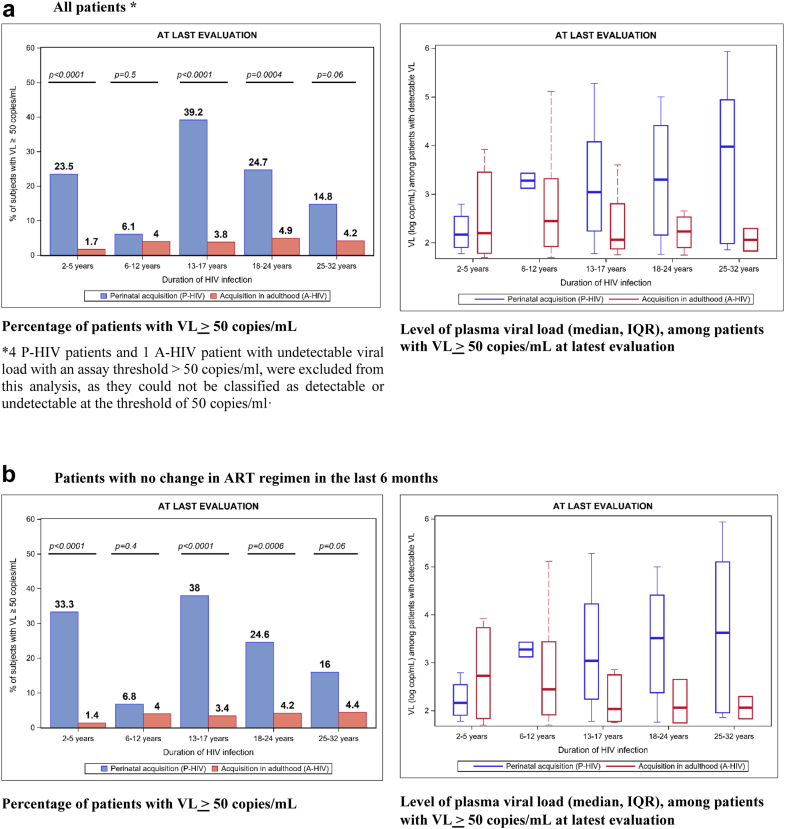
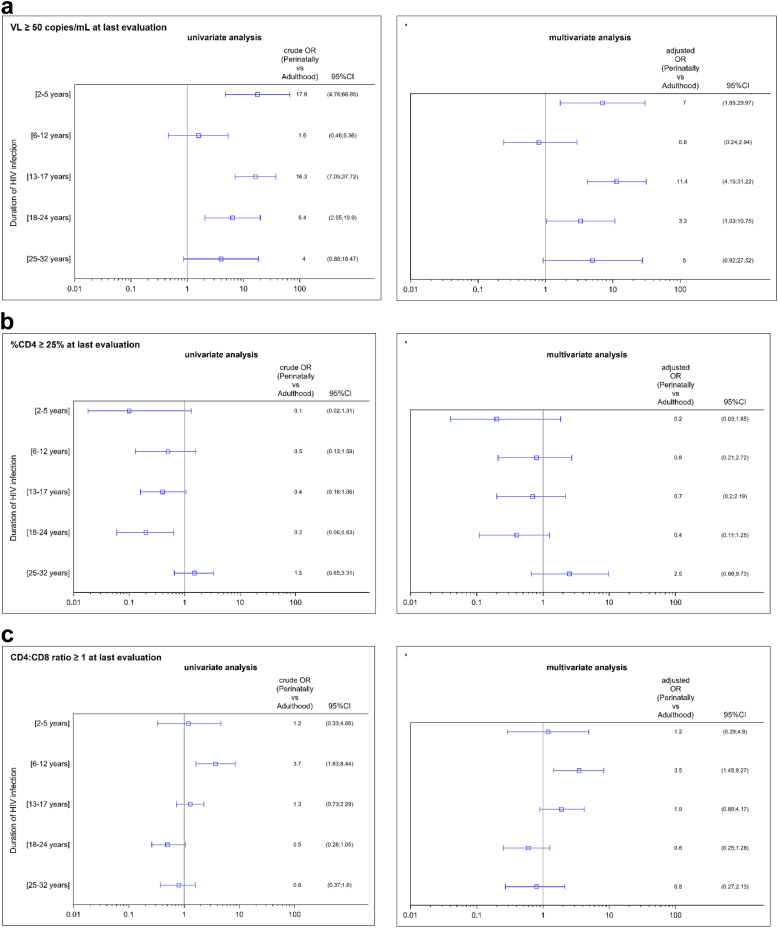
Findings: 310 P-HIV were compared to 1515 A-HIV (median current ages 20.9 [IQR:14.4-25.5] and 45.9 [IQR:37.9-53.5] respectively). VF at the time of the most recent evaluation was significantly higher among P-HIV (22.6%, 69/306) than A-HIV (3.3%, 50/1514); p ≤ 0.0001. The risk of VF was particularly high among the youngest children (2-5 years), adolescents (13-17 years) and young adults (18-24 years), compared to A-HIV with a similar duration of infection: adjusted Odds-Ratio (aOR) 7.0 [95% CI: 1.7; 30.0], 11.4 [4.2; 31.2] and 3.3 [1.0; 10.8] respectively. The level of CD4 cell percentages did not differ between P-HIV and A-HIV. P-HIV aged 6-12 and 13-17 were more likely than A-HIV to have a CD4:CD8 ratio ≥ 1: 84.1% vs. 58.8% (aOR = 3.5 [1.5; 8.3]), and 60.9% vs. 54.7% (aOR = 1.9 [0.9; 4.2]) respectively.
Interpretation: P-HIV were at a higher risk of VF than A-HIV with a similar duration of infection, even after adjusting for treatment history, whereas they were not at a higher risk of immunological impairment. Exposure to viral replication among young patients living with HIV since birth or a very early age, probably because of lower adherence, could have an impact on health, raising major concerns about the selection of resistance mutations and the risk of HIV transmission.
Funding: Inserm - ANRS MIE.
Keywords: Cohort; Epidemiology; Immunological outcome; Perinatal HIV infection; Viral failure.
© 2024 Published by Elsevier Ltd.
Conflict of interest statement
LM has received grants from ANRS-MIE, SIDACTION, all of which were paid to her institution. PF has received grants from ANRS-MIE which were paid to his institution, personal fees from MSD France, ViiV Healthcare, Janssen Cilag Gilead Sciences, support for attending meetings/and or travel from MSD France, Gilead Sciences, ViiV Healthcare. PF reports to be EACS Panel member. RS has received grants from ANRS-MIE which were paid to her institution. JW has received grants from ANRS-MIE and Region Ile de France, all of which were paid to her institution. All other authors declare no competing interests.
Figures
References
-
- de Martino M., Tovo P.A., Balducci M., et al. Reduction in mortality with availability of antiretroviral therapy for children with perinatal HIV-1 infection. Italian Register for HIV Infection in Children and the Italian National AIDS Registry. JAMA. 2000;284:190–197. - PubMed
-
- Gortmaker S.L., Hughes M., Cervia J., et al. Effect of combination therapy including protease inhibitors on mortality among children and adolescents infected with HIV-1. N Engl J Med. 2001;345:1522–1528. - PubMed
-
- Sánchez J.M., Ramos Amador J.T., Fernández de Miguel S., et al. Impact of highly active antiretroviral therapy on the morbidity and mortality in Spanish human immunodeficiency virus infected children. Pediatr Infect Dis J. 2003;22:863–867. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
