

Variation in Sedative and Analgesic Use During the COVID-19 Pandemic and Associated Outcomes
- PMID: 38576856
- PMCID: PMC10994221
- DOI: 10.1016/j.chstcc.2024.100047
Variation in Sedative and Analgesic Use During the COVID-19 Pandemic and Associated Outcomes
Abstract
Background: Providing analgesia and sedation is an essential component of caring for many mechanically ventilated patients. The selection of analgesic and sedative medications during the COVID-19 pandemic, and the impact of these sedation practices on patient outcomes, remain incompletely characterized.
Research question: What were the hospital patterns of analgesic and sedative use for patients with COVID-19 who received mechanical ventilation (MV), and what differences in clinical patient outcomes were observed across prevailing sedation practices?
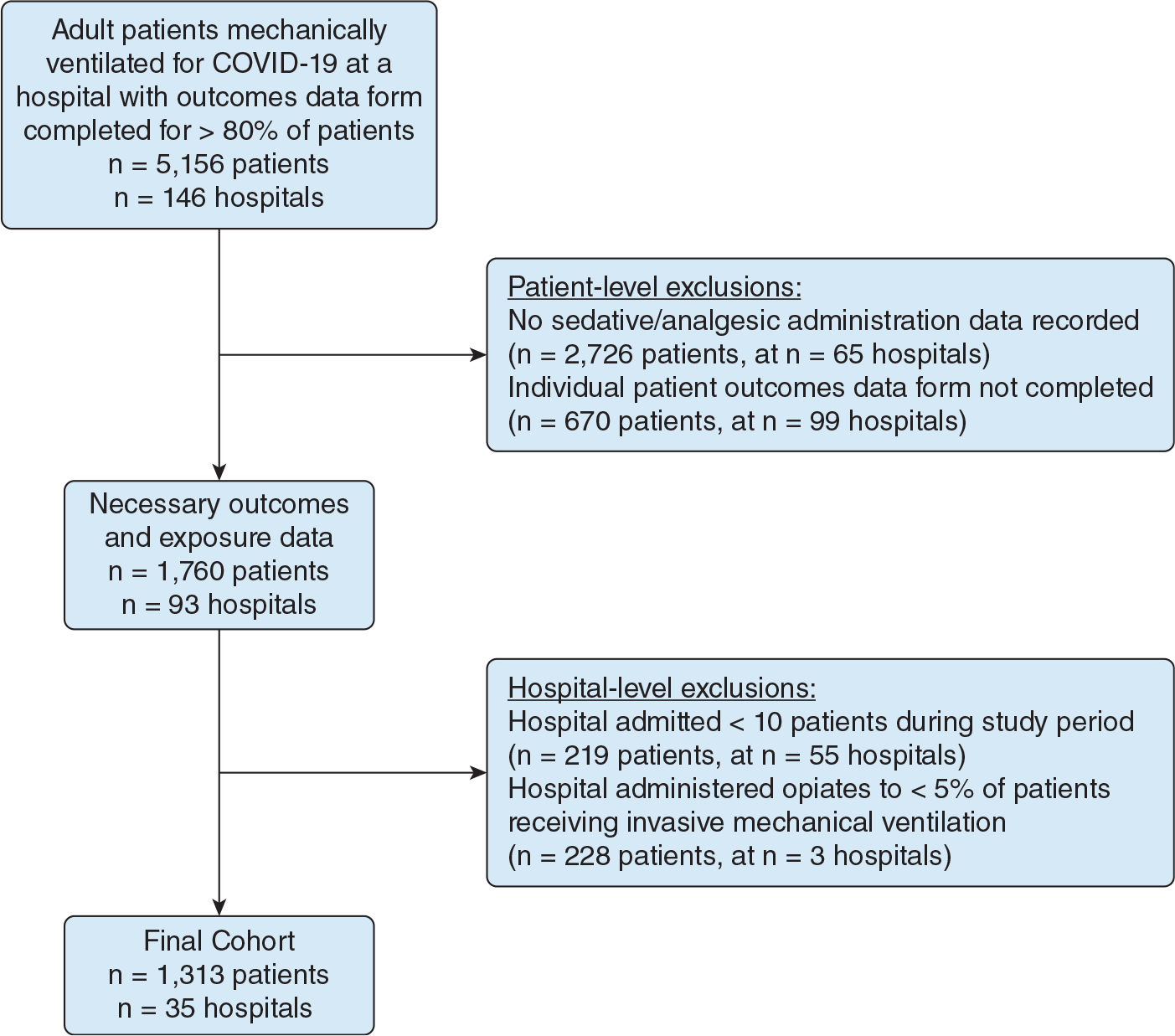
Study design and methods: We conducted an observational cohort study of hospitalized adults who received MV for COVID-19 from February 2020 through April 2021 within the Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study (VIRUS) COVID-19 Registry. To describe common sedation practices, we used hierarchical clustering to group hospitals based on the percentage of patients who received various analgesic and sedative medications. We then used multivariable regression models to evaluate the association between hospital analgesia and sedation cluster and duration of MV (with a placement of death [POD] approach to account for competing risks).
Results: We identified 1,313 adults across 35 hospitals admitted with COVID-19 who received MV. Two clusters of analgesia and sedation practices were identified. Cluster 1 hospitals generally administered opioids and propofol with occasional use of additional sedatives (eg, benzodiazepines, alpha-agonists, and ketamine); cluster 2 hospitals predominantly used opioids and benzodiazepines without other sedatives. As compared with patients in cluster 2, patients admitted to cluster 1 hospitals underwent a shorter adjusted median duration of MV with POD (β-estimate, -5.9; 95% CI, -11.2 to -0.6; P = .03).
Interpretation: Patients who received MV for COVID-19 in hospitals that prioritized opioids and propofol for analgesia and sedation experienced shorter adjusted median duration of MV with POD as compared with patients who received MV in hospitals that primarily used opioids and benzodiazepines.
Keywords: COVID-19; acute respiratory failure; analgesia; mechanical ventilation; sedation.
Figures
References
-
- Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e873. - PubMed
-
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000. May;342(20):1471–1477. - PubMed
-
- Treggiari MM, Romand JA, Yanez ND, et al. Randomized trial of light versus deep sedation on mental health after critical illness*. Crit Care Med. 2009;37(9):2527–2534. - PubMed
-
- Girard TD, Kress JP, Fuchs BD, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008. Jan 12;371(9607):126–134. - PubMed
-
- Kollef MH, Levy NT, Ahrens TS, Schaiff R, Prentice D, Sherman G. The use of continuous IV sedation is associated with prolongation of mechanical ventilation. Chest. 1998;114(2):541–548. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous