

Mucinous neoplasm of the appendix: A case report and review of literature
- PMID: 38577069
- PMCID: PMC10989352
- DOI: 10.4240/wjgs.v16.i3.944
Mucinous neoplasm of the appendix: A case report and review of literature
Abstract
Background: Appendiceal mucinous neoplasms (AMNs), although not classified as rare, are relatively uncommon tumors most often discovered incidentally during colorectal surgery. Accurate identification of AMNs is difficult due to non-specific symptoms, overlapping tumor markers with other conditions, and the potential for misdiagnosis. This underscores the urgent need for precision in diagnosis to prevent severe complications.
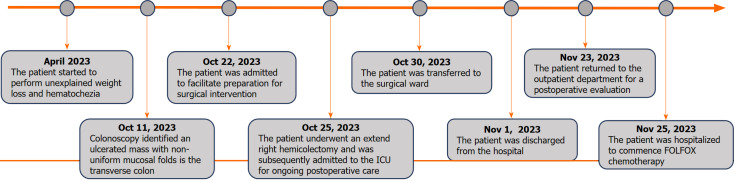
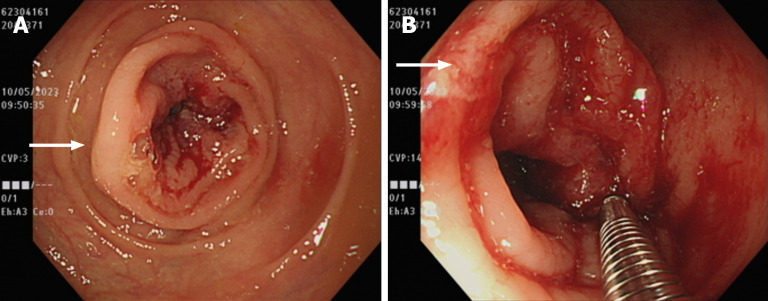
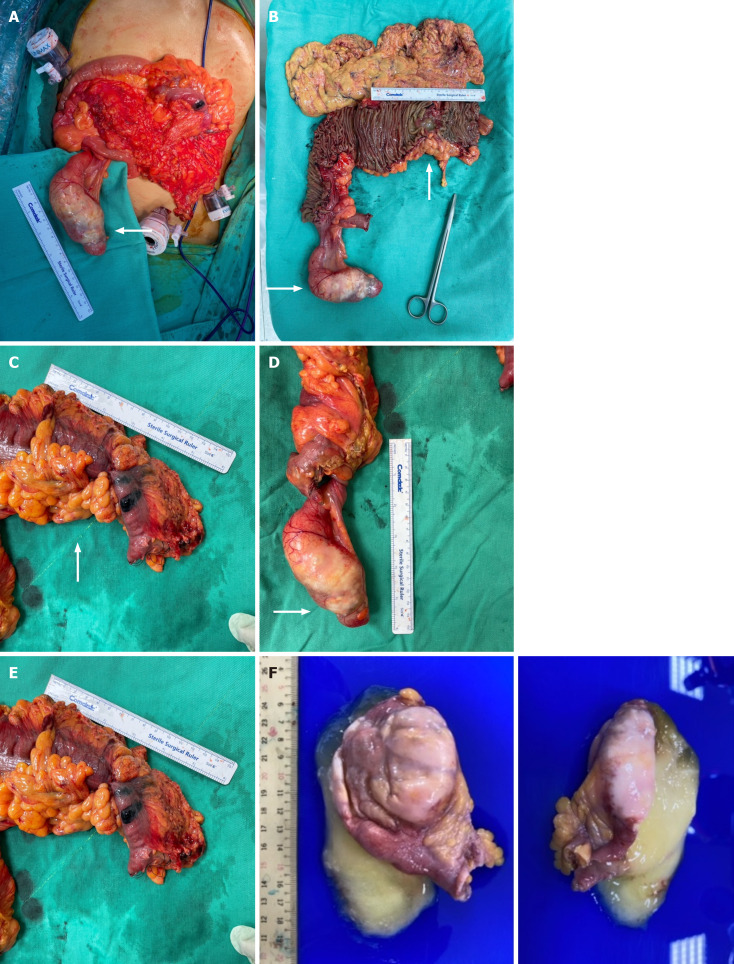
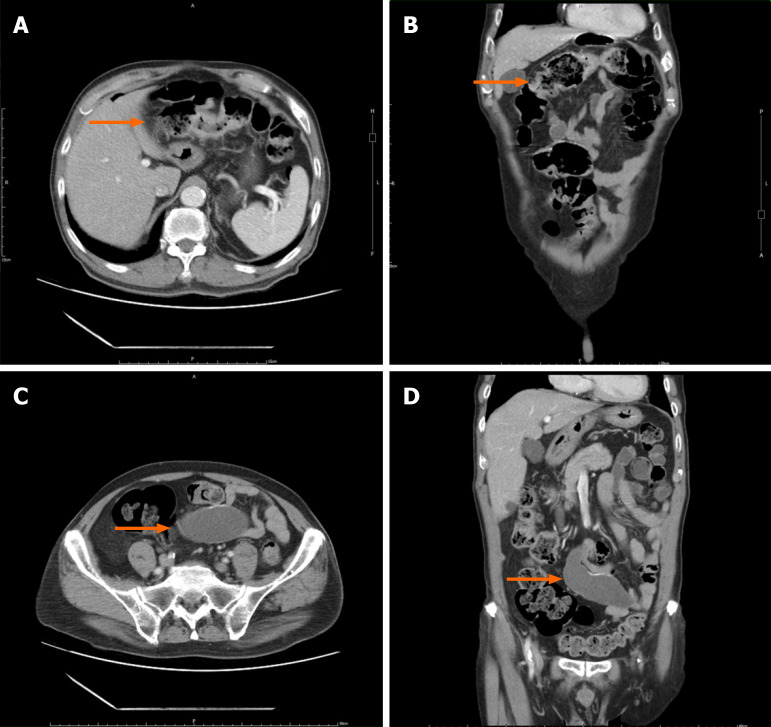
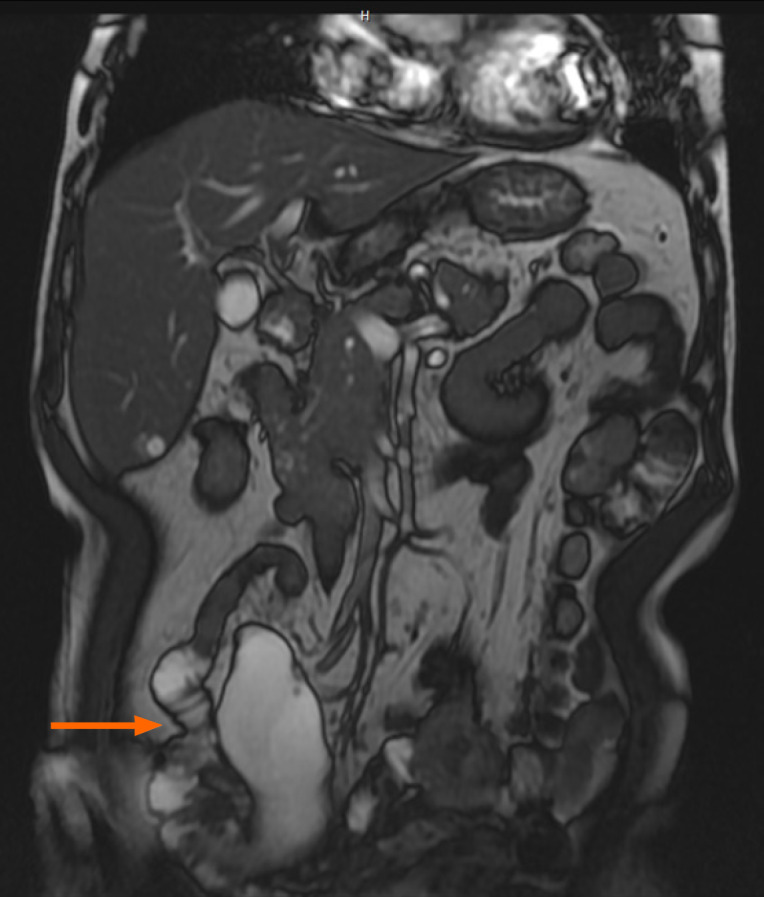
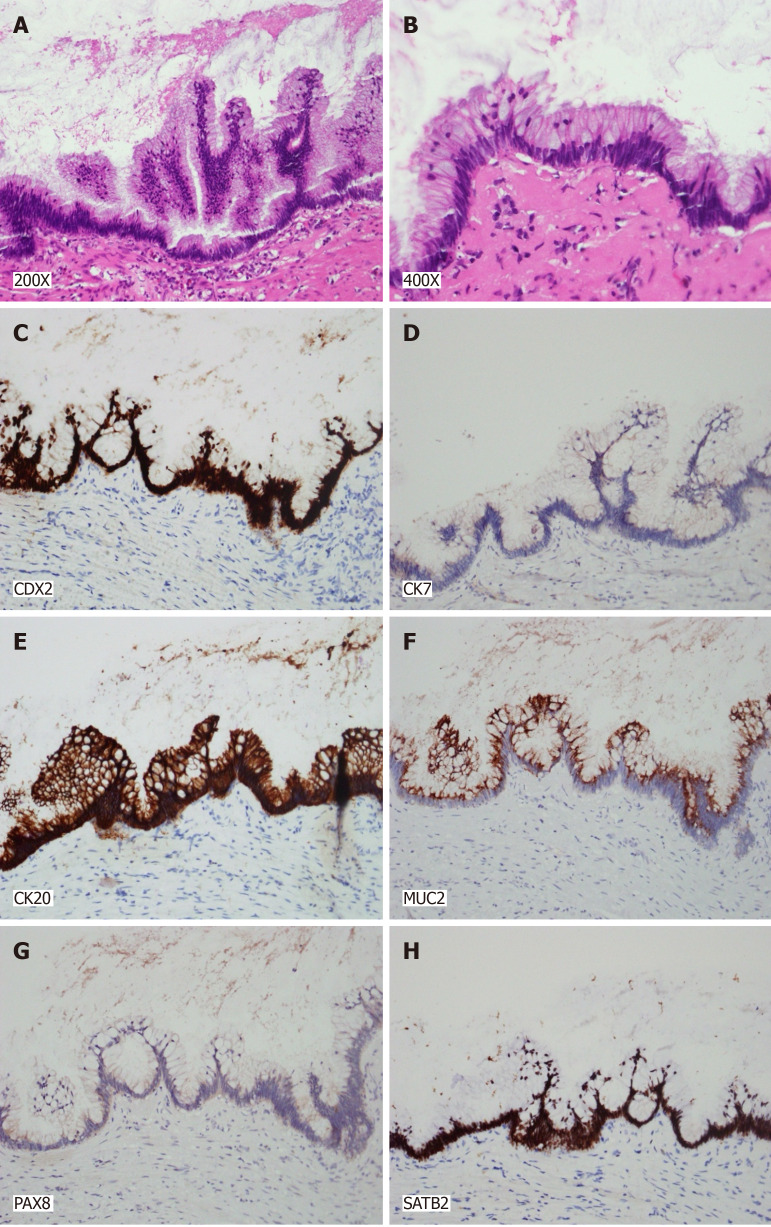
Case summary: This case report describes the unexpected discovery and treatment of a low-grade AMN (LAMN) in a 74-year-old man undergoing laparoscopic hemicolectomy for transverse colon adenocarcinoma (AC). Preoperatively, non-specific gastrointestinal symptoms and elevated tumor markers masked the presence of AMN. The tumor, presumed to be an AMN peritoneal cyst intraoperatively, was confirmed as LAMN through histopathological examination. The neoplasm exhibited mucin accumulation and a distinct immunohistochemical profile: Positive for Homeobox protein CDX-2, Cytokeratin 20, special AT-rich sequence-binding protein 2, and Mucin 2 but negative for cytokeratin 7 and Paired box gene 8. This profile aids in distinguishing appendiceal and ovarian mucinous tumors. Postoperative recovery was uncomplicated, and the patient initiated adjuvant chemotherapy for the colon AC.
Conclusion: This case highlights the diagnostic complexity of AMNs, emphasizing the need for vigilant identification to avert potential complications, such as pseudomyxoma peritonei.
Keywords: Adenocarcinoma; Appendiceal neoplasms; Case report; Low-grade appendiceal mucinous neoplasm; Peritoneal neoplasms; Pseudomyxoma peritonei.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflicts of interest to disclose.
Figures
Similar articles
-
Appendiceal Mucinous Neoplasm: A Case of an Incidental Finding.Cureus. 2024 May 2;16(5):e59540. doi: 10.7759/cureus.59540. eCollection 2024 May. Cureus. 2024. PMID: 38826949 Free PMC article.
-
Pseudomyxoma peritonei and selected other aspects of the spread of appendiceal neoplasms.Semin Diagn Pathol. 2004 May;21(2):134-50. doi: 10.1053/j.semdp.2004.12.002. Semin Diagn Pathol. 2004. PMID: 15807473 Review.
-
Low-grade appendiceal mucinous neoplasm associated with Urothelial carcinoma: A rare case report from Syria.Ann Med Surg (Lond). 2022 Mar 29;76:103525. doi: 10.1016/j.amsu.2022.103525. eCollection 2022 Apr. Ann Med Surg (Lond). 2022. PMID: 35495395 Free PMC article.
-
Diagnostic difficulties in the differentiation between an ovarian metastatic low‑grade appendiceal mucinous neoplasm and primary ovarian mucinous cancer: A case report and literature review.Oncol Lett. 2024 Aug 16;28(5):500. doi: 10.3892/ol.2024.14633. eCollection 2024 Nov. Oncol Lett. 2024. PMID: 39233821 Free PMC article.
-
Appendiceal Mucinous Neoplasm: Nurse Education About a Rare and Complex Disease.Clin J Oncol Nurs. 2020 Aug 1;24(4):409-414. doi: 10.1188/20.CJON.409-414. Clin J Oncol Nurs. 2020. PMID: 32678367 Review.
References
-
- Yakan S, Caliskan C, Uguz A, Korkut M, Çoker A. A Retrospective Study on Mucocele of the Appendix Presented with Acute Abdomen or Acute Appendicitis. Hong Kong J Emerg Med. 2011;18:144–149.
-
- Minni F, Petrella M, Morganti A, Santini D, Marrano D. Giant mucocele of the appendix: report of a case. Dis Colon Rectum. 2001;44:1034–1036. - PubMed
-
- Fujiwara T, Hizuta A, Iwagaki H, Matsuno T, Hamada M, Tanaka N, Orita K. Appendiceal mucocele with concomitant colonic cancer. Report of two cases. Dis Colon Rectum. 1996;39:232–236. - PubMed
-
- McCusker ME, Coté TR, Clegg LX, Sobin LH. Primary malignant neoplasms of the appendix: a population-based study from the surveillance, epidemiology and end-results program, 1973-1998. Cancer. 2002;94:3307–3312. - PubMed
-
- COLLINS DC. 71,000 HUMAN APPENDIX SPECIMENS. A FINAL REPORT, SUMMARIZING FORTY YEARS' STUDY. Am J Proctol. 1963;14:265–281. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
