

Role of ablation therapy in conjunction with surgical resection for neuroendocrine tumors involving the liver
- PMID: 38577070
- PMCID: PMC10989351
- DOI: 10.4240/wjgs.v16.i3.768
Role of ablation therapy in conjunction with surgical resection for neuroendocrine tumors involving the liver
Abstract
Background: Resection of hepatic metastasis from neuroendocrine tumors (NETs) improves quality of life and prolongs 5-year survival. Ablation can be utilized with surgery to achieve complete resection. Although several studies report long-term outcomes for patients undergoing ablation, none have explored perioperative effects of ablation in patients with metastatic NETs.
Aim: To determine if intra-operative ablation during hepatectomy increases risk of adverse outcomes such as surgical site infections (SSIs), bleeding, and bile leak.
Methods: A retrospective analysis of the hepatectomy National Surgical Quality Improvement Program database from 2015-2019 was performed to determine the odds of SSIs, bile leaks, or bleeding in patients undergoing intraoperative ablation when compared to hepatectomy alone.
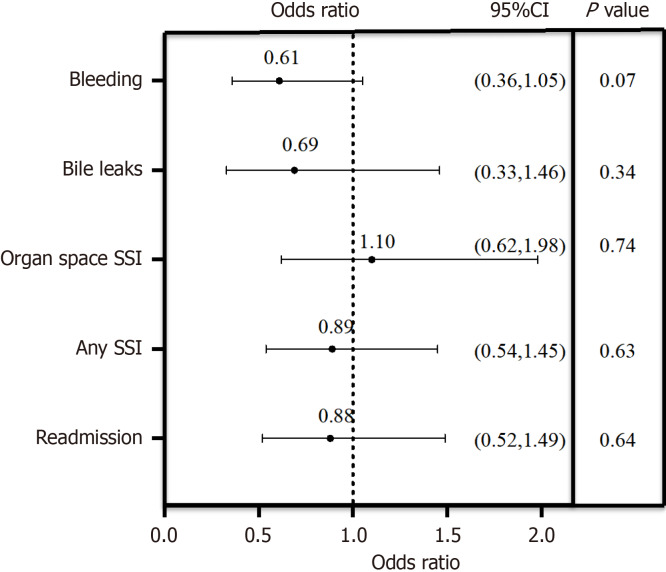
Results: Of the 966 patients included in the study, 298 (30.9%) underwent ablation during hepatectomy. There were 78 (11.7%) patients with SSIs in the hepatectomy alone group and 39 (13.1%) patients with a SSIs in the hepatectomy with ablation group. Bile leak occurred in 41 (6.2%) and 14 (4.8%) patients in the two groups, respectively; bleeding occurred in 117 (17.5%) and 33 (11.1%), respectively. After controlling for confounding variables, ablation did not increase risk of SSI (P = 0.63), bile leak (P = 0.34) or bleeding (P = 0.07) when compared to patients undergoing resection alone on multivariate analysis.
Conclusion: Intraoperative ablation with hepatic resection for NETs is safe in the perioperative period without significant increased risk of infection, bleeding, or bile leak. Surgeons should utilize this modality when appropriate to achieve optimal disease control and outcomes.
Keywords: Ablation; Bile leaks; Bleeding; Hepatectomy; Neuroendocrine tumor; Surgical site infections.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Hepatic surgery for metastases from neuroendocrine tumors.Surg Oncol Clin N Am. 2003 Jan;12(1):231-42. doi: 10.1016/s1055-3207(02)00076-5. Surg Oncol Clin N Am. 2003. PMID: 12735141 Review.
-
Role of Drain Placement in Major Hepatectomy: A NSQIP Analysis of Procedure-Targeted Hepatectomy Cases.World J Surg. 2017 Apr;41(4):1110-1118. doi: 10.1007/s00268-016-3750-4. World J Surg. 2017. PMID: 27738836
-
Concurrent major hepatic resection with primary colorectal cancer increases risk of organ space infections.Surg Endosc. 2023 Apr;37(4):2908-2914. doi: 10.1007/s00464-022-09810-w. Epub 2022 Dec 12. Surg Endosc. 2023. PMID: 36508007
-
Patterns of care among patients undergoing hepatic resection: a query of the National Surgical Quality Improvement Program-targeted hepatectomy database.J Surg Res. 2015 Jun 15;196(2):221-8. doi: 10.1016/j.jss.2015.02.016. Epub 2015 Mar 19. J Surg Res. 2015. PMID: 25881789
-
Surgical management of pancreatic neuroendocrine liver metastases.J Gastrointest Oncol. 2020 Jun;11(3):590-600. doi: 10.21037/jgo.2019.11.02. J Gastrointest Oncol. 2020. PMID: 32655938 Free PMC article. Review.
References
-
- Proye C. Natural history of liver metastasis of gastroenteropancreatic neuroendocrine tumors: place for chemoembolization. World J Surg. 2001;25:685–688. - PubMed
-
- Knox CD, Anderson CD, Lamps LW, Adkins RB, Pinson CW. Long-term survival after resection for primary hepatic carcinoid tumor. Ann Surg Oncol. 2003;10:1171–1175. - PubMed
-
- Vogl TJ, Naguib NN, Zangos S, Eichler K, Hedayati A, Nour-Eldin NE. Liver metastases of neuroendocrine carcinomas: interventional treatment via transarterial embolization, chemoembolization and thermal ablation. Eur J Radiol. 2009;72:517–528. - PubMed
-
- Mulier S, Mulier P, Ni Y, Miao Y, Dupas B, Marchal G, De Wever I, Michel L. Complications of radiofrequency coagulation of liver tumours. Br J Surg. 2002;89:1206–1222. - PubMed
LinkOut - more resources
Full Text Sources
