

N-glycan biosignatures as a potential diagnostic biomarker for early-stage pancreatic cancer
- PMID: 38577461
- PMCID: PMC10989390
- DOI: 10.4251/wjgo.v16.i3.659
N-glycan biosignatures as a potential diagnostic biomarker for early-stage pancreatic cancer
Abstract
Background: Pancreatic ductal adenocarcinoma (PDAC) has a poor prognosis, with a 5-year survival rate of less than 10%, owing to its late-stage diagnosis. Early detection of pancreatic cancer (PC) can significantly increase survival rates.
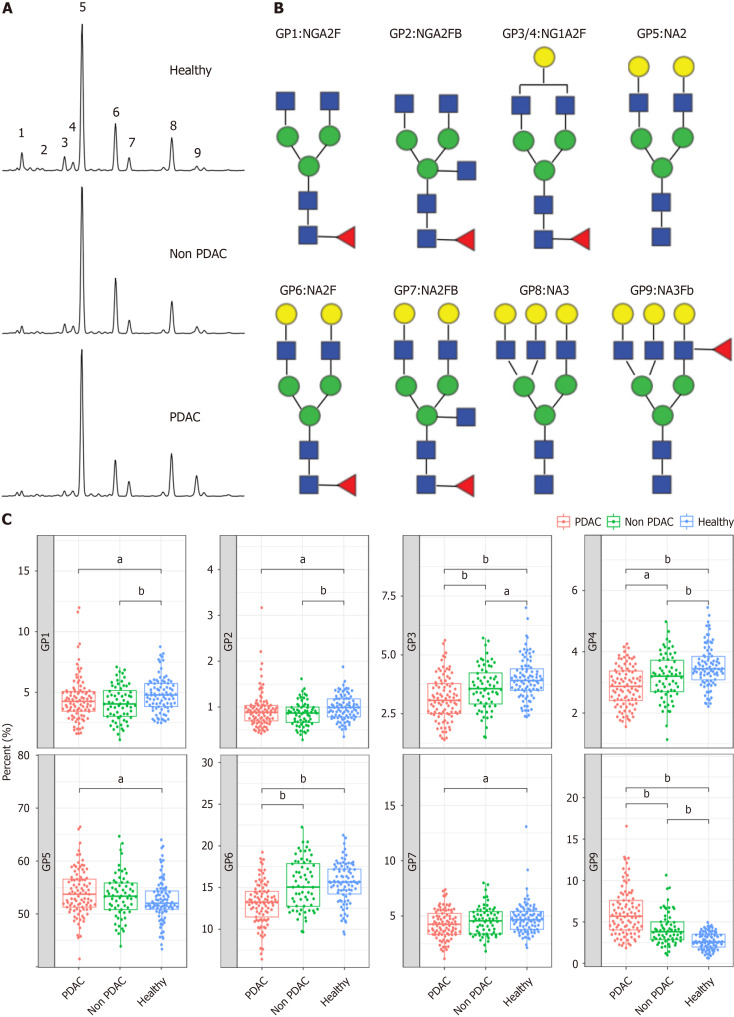
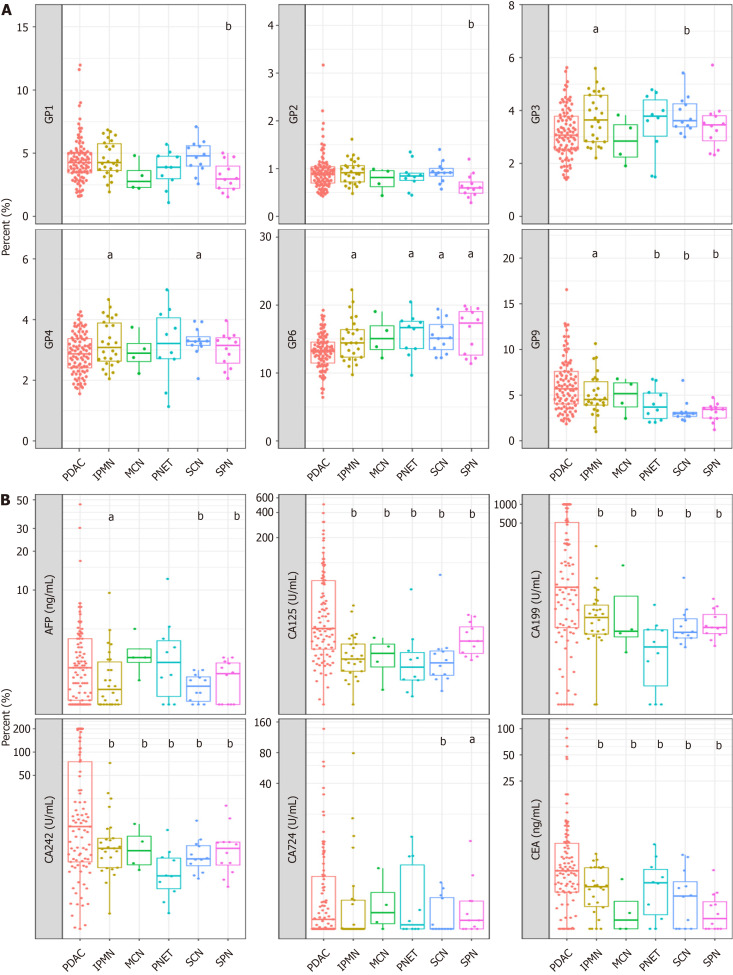
Aim: To identify the serum biomarker signatures associated with early-stage PDAC by serum N-glycan analysis.
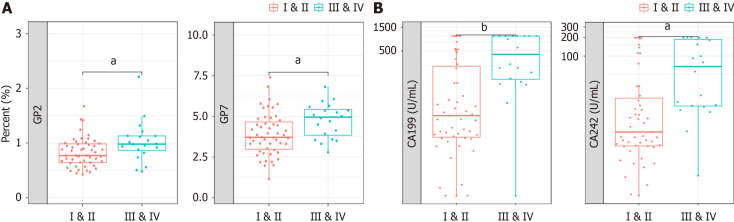
Methods: An extensive patient cohort was used to determine a biomarker signature, including patients with PDAC that was well-defined at an early stage (stages I and II). The biomarker signature was derived from a case-control study using a case-cohort design consisting of 29 patients with stage I, 22 with stage II, 4 with stage III, 16 with stage IV PDAC, and 88 controls. We used multiparametric analysis to identify early-stage PDAC N-glycan signatures and developed an N-glycan signature-based diagnosis model called the "Glyco-model".
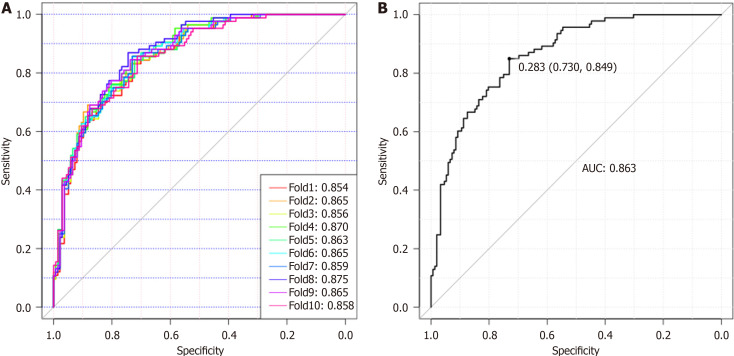
Results: The biomarker signature was created to discriminate samples derived from patients with PC from those of controls, with a receiver operating characteristic area under the curve of 0.86. In addition, the biomarker signature combined with cancer antigen 19-9 could discriminate patients with PDAC from controls, with a receiver operating characteristic area under the curve of 0.919. Glyco-model demonstrated favorable diagnostic performance in all stages of PC. The diagnostic sensitivity for stage I PDAC was 89.66%.
Conclusion: In a prospective validation study, this serum biomarker signature may offer a viable method for detecting early-stage PDAC.
Keywords: Biomarkers; Glycomics; N-glycans; Pancreatic cancer; Predictive modeling.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7–33. - PubMed
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17–48. - PubMed
-
- Walter FM, Mills K, Mendonça SC, Abel GA, Basu B, Carroll N, Ballard S, Lancaster J, Hamilton W, Rubin GP, Emery JD. Symptoms and patient factors associated with diagnostic intervals for pancreatic cancer (SYMPTOM pancreatic study): a prospective cohort study. Lancet Gastroenterol Hepatol. 2016;1:298–306. - PMC - PubMed
LinkOut - more resources
Full Text Sources
