

Efficacy and safety of perioperative therapy for locally resectable gastric cancer: A network meta-analysis of randomized clinical trials
- PMID: 38577462
- PMCID: PMC10989386
- DOI: 10.4251/wjgo.v16.i3.1046
Efficacy and safety of perioperative therapy for locally resectable gastric cancer: A network meta-analysis of randomized clinical trials
Abstract
Background: Gastric cancer (GC) is the fifth most commonly diagnosed malignancy worldwide, with over 1 million new cases per year, and the third leading cause of cancer-related death.
Aim: To determine the optimal perioperative treatment regimen for patients with locally resectable GC.
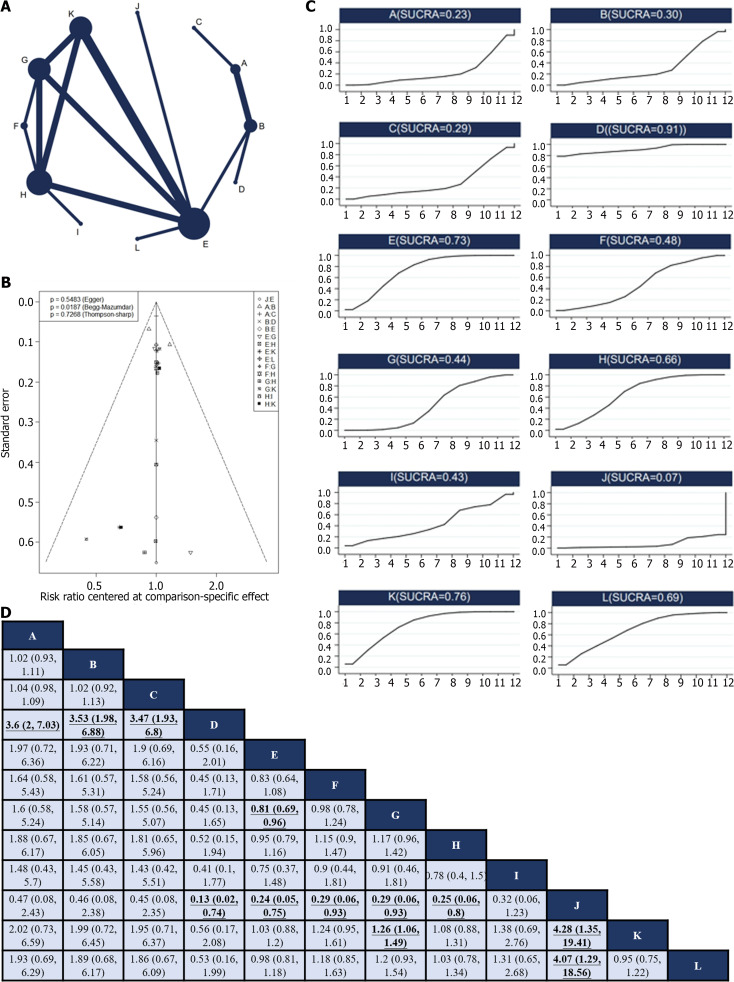
Methods: A comprehensive literature search was conducted, focusing on phase II/III randomized controlled trials (RCTs) assessing perioperative chemotherapy and chemoradiotherapy in treating locally resectable GC. The R0 resection rate, overall survival (OS), disease-free survival (DFS), and incidence of grade 3 or higher nonsurgical severe adverse events (SAEs) associated with various perioperative regimens were analyzed. A Bayesian network meta-analysis was performed to compare treatment regimens and rank their efficacy.
Results: Thirty RCTs involving 8346 patients were included in this study. Neoadjuvant XELOX plus neoadjuvant radiotherapy and neoadjuvant CF were found to significantly improve the R0 resection rate compared with surgery alone, and the former had the highest probability of being the most effective option in this context. Neoadjuvant plus adjuvant FLOT was associated with the highest probability of being the best regimen for improving OS. Owing to limited data, no definitive ranking could be determined for DFS. Considering nonsurgical SAEs, FLO has emerged as the safest treatment regimen.
Conclusion: This study provides valuable insights for clinicians when selecting perioperative treatment regimens for patients with locally resectable GC. Further studies are required to validate these findings.
Keywords: Efficacy and safety; Gastric cancer; Network meta-analysis; Perioperative treatment.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Authors have no conflicts of interest to declare.
Figures



Similar articles
-
Comparative Effectiveness of Neoadjuvant Treatments for Resectable Gastroesophageal Cancer: A Network Meta-Analysis.Front Pharmacol. 2018 Aug 6;9:872. doi: 10.3389/fphar.2018.00872. eCollection 2018. Front Pharmacol. 2018. PMID: 30127746 Free PMC article.
-
The Efficacy and Safety of (Neo)Adjuvant Therapy for Gastric Cancer: A Network Meta-analysis.Cancers (Basel). 2019 Jan 11;11(1):80. doi: 10.3390/cancers11010080. Cancers (Basel). 2019. PMID: 30641964 Free PMC article.
-
Perioperative treatment in resectable gastric cancer with spartalizumab in combination with fluorouracil, leucovorin, oxaliplatin and docetaxel (FLOT): a phase II study (GASPAR).BMC Cancer. 2022 May 12;22(1):537. doi: 10.1186/s12885-022-09623-z. BMC Cancer. 2022. PMID: 35549674 Free PMC article. Clinical Trial.
-
Comparison of neoadjuvant regimens for resectable gastroesophageal junction cancer: a systematic review of randomized clinical trials across three decades.J Gastrointest Oncol. 2022 Jun;13(3):1454-1466. doi: 10.21037/jgo-22-29. J Gastrointest Oncol. 2022. PMID: 35837173 Free PMC article. Review.
-
Evaluation of neoadjuvant immunotherapy plus chemotherapy in Chinese surgically resectable gastric cancer: a pilot study by meta-analysis.Front Immunol. 2023 Jun 23;14:1193614. doi: 10.3389/fimmu.2023.1193614. eCollection 2023. Front Immunol. 2023. PMID: 37426646 Free PMC article.
Cited by
-
Prognostic Value and Therapeutic Significance of CCL Chemokines in Gastric Cancer.Curr Med Chem. 2024;31(42):7043-7058. doi: 10.2174/0109298673315146240731100101. Curr Med Chem. 2024. PMID: 39129286
References
-
- Ajani JA, D'Amico TA, Bentrem DJ, Chao J, Cooke D, Corvera C, Das P, Enzinger PC, Enzler T, Fanta P, Farjah F, Gerdes H, Gibson MK, Hochwald S, Hofstetter WL, Ilson DH, Keswani RN, Kim S, Kleinberg LR, Klempner SJ, Lacy J, Ly QP, Matkowskyj KA, McNamara M, Mulcahy MF, Outlaw D, Park H, Perry KA, Pimiento J, Poultsides GA, Reznik S, Roses RE, Strong VE, Su S, Wang HL, Wiesner G, Willett CG, Yakoub D, Yoon H, McMillian N, Pluchino LA. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20:167–192. - PubMed
-
- Yang L, Kartsonaki C, Millwood IY, Chen Z. Helicobacter pylori infection and risk of gastric cancer - Authors' reply. Lancet Public Health. 2022;7:e303. - PubMed
-
- Hatakeyama M. Malignant Helicobacter pylori-Associated Diseases: Gastric Cancer and MALT Lymphoma. Advances in Experimental Medicine and Biology. 2019;1149:135–149. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
