

Machine Learning-based Development and Validation of a Cell Senescence Predictive and Prognostic Signature in Intrahepatic Cholangiocarcinoma
- PMID: 38577599
- PMCID: PMC10988306
- DOI: 10.7150/jca.92698
Machine Learning-based Development and Validation of a Cell Senescence Predictive and Prognostic Signature in Intrahepatic Cholangiocarcinoma
Abstract
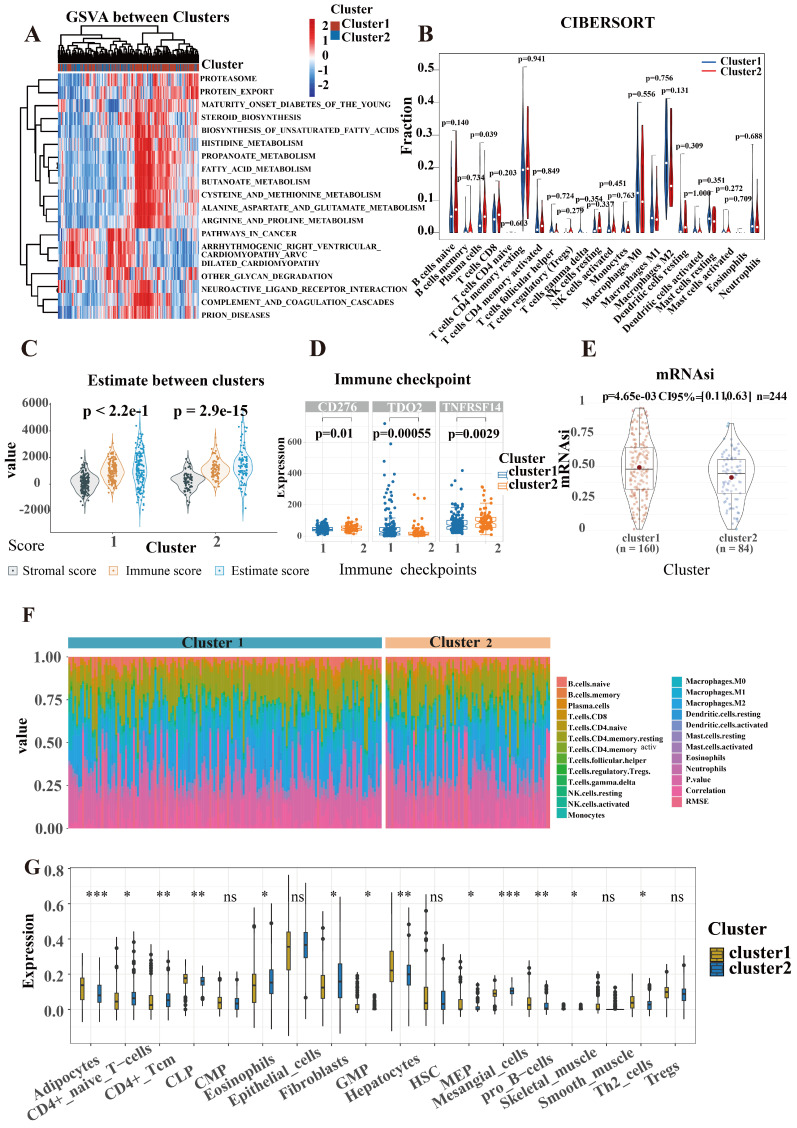
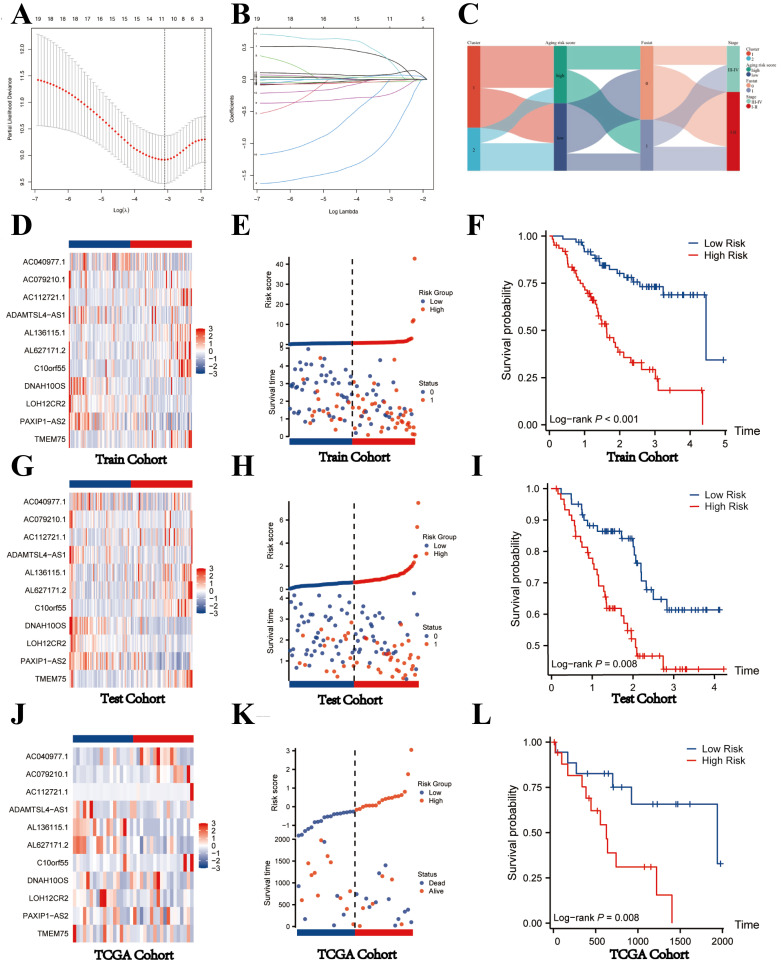
Background: Previous studies have shown that cellular senescence is strongly associated with tumorigenesis and the tumor microenvironment. Accordingly, we developed a novel prognostic signature for intrahepatic cholangiocarcinoma (ICCA) based on senescence-associated long non-coding RNAs (SR-lncRNAs) and identified a lncRNA-miRNA-mRNA axis involving in ICCA. Methods: Based on the 197 senescence-associated genes (SRGs) from Genacards and their expression in Fu-ICCA cohort, we identified 20 lncRNAs as senescence-associated lncRNAs (SR-lncRNAs) through co-expression and cox-regression analysis. According to 20 SR-lncRNAs, patients with ICCA were classified into 2 molecular subtypes using unsupervised clustering machine learning approach and to explore the prognostic and functional heterogeneity between these two subtypes. Subsequently, we integrated 113 machine learning algorithms to develop senescence-related lncRNA signature, ultimately identifying 11 lncRNAs and constructing prognostic models and risk stratification. The correlation between the signature and the immune landscape, immunotherapy response as well as drug sensitivity are explored too. Results: We developed a novel senescence related signature. The predictive model and risk score calculated by the signature exhibited favorable prognostic predictive performance, which is a suitable independent risk factor for the prognosis of patients with ICCA based on Kaplan-Meier plotter, nomogram and receiving operating characteristic (ROC) curves. The results were validated using external datasets. Estimate, ssGSEA (single sample gene set enrichment analysis), IPS (immunophenotype score) and TIDE (tumor immune dysfunction and exclusion) algorithms revealed higher immune infiltration, higher immune scores, lower immune escape potential and better response to immunotherapy in the high-risk group. In addition, signature identifies eight chemotherapeutic agents, including cisplatin for patients with different risk levels, providing guidance for clinical treatment. Finally, we identified a set of lncRNA-miRNA-mRNA axes involved in ICCA through regulation of senescence. Conclusion: SR-lncRNAs signature can favorably predict the prognosis, risk stratification, immune landscape and immunotherapy response of patients with ICCA and consequently guide individualized treatment.
Keywords: cellular senescence; cholangiocarcinoma; long non-coding RNAs (lncRNAs); machine learning; signature.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures







Similar articles
-
A metabolism-related 4-lncRNA prognostic signature and corresponding mechanisms in intrahepatic cholangiocarcinoma.BMC Cancer. 2021 May 25;21(1):608. doi: 10.1186/s12885-021-08322-5. BMC Cancer. 2021. PMID: 34034689 Free PMC article.
-
Identification of a novel cellular senescence-related lncRNA signature for prognosis and immune response in osteosarcoma.Transl Cancer Res. 2024 Jul 31;13(7):3742-3759. doi: 10.21037/tcr-24-163. Epub 2024 Jul 8. Transl Cancer Res. 2024. PMID: 39145087 Free PMC article.
-
Development and experimental validation of a senescence-related long non-coding RNA signature for prognostic prediction and immune microenvironment characterization in gastric cancer patients.J Gastrointest Oncol. 2024 Dec 31;15(6):2413-2436. doi: 10.21037/jgo-24-792. Epub 2024 Dec 26. J Gastrointest Oncol. 2024. PMID: 39816024 Free PMC article.
-
Genetic/Epigenetic Alteration and Tumor Immune Microenvironment in Intrahepatic Cholangiocarcinoma: Transforming the Immune Microenvironment with Molecular-Targeted Agents.Liver Cancer. 2023 Oct 4;13(2):136-149. doi: 10.1159/000534443. eCollection 2024 Apr. Liver Cancer. 2023. PMID: 38751556 Free PMC article. Review.
-
Unveil Intrahepatic Cholangiocarcinoma Heterogeneity through the Lens of Omics and Multi-Omics Approaches.Cancers (Basel). 2024 Aug 20;16(16):2889. doi: 10.3390/cancers16162889. Cancers (Basel). 2024. PMID: 39199659 Free PMC article. Review.
Cited by
-
Identification of the shared gene signatures in retinoblastoma and osteosarcoma by machine learning.Sci Rep. 2024 Dec 28;14(1):31355. doi: 10.1038/s41598-024-82789-7. Sci Rep. 2024. PMID: 39733097 Free PMC article.
-
Nomogram for Predicting Survival Post-Immune Therapy in Cholangiocarcinoma Based on Inflammatory Biomarkers.Cancer Control. 2024 Jan-Dec;31:10732748241305237. doi: 10.1177/10732748241305237. Cancer Control. 2024. PMID: 39638310 Free PMC article.
-
New Relevant Evidence in Cholangiocarcinoma Biology and Characterization.Cancers (Basel). 2024 Dec 19;16(24):4239. doi: 10.3390/cancers16244239. Cancers (Basel). 2024. PMID: 39766138 Free PMC article. Review.
References
-
- Cong W-M, Wu M-C. New insights into molecular diagnostic pathology of primary liver cancer: Advances and challenges. Cancer Lett. 2015;368:14–9. - PubMed
-
- Calcinotto A, Kohli J, Zagato E, Pellegrini L, Demaria M, Alimonti A. Cellular Senescence: Aging, Cancer, and Injury. Physiol Rev. 2019;99:1047–78. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
