

Changes of uterocervical angle and cervical length in early and mid-pregnancy and their value in predicting spontaneous preterm birth
- PMID: 38577623
- PMCID: PMC10991810
- DOI: 10.3389/fphys.2024.1304513
Changes of uterocervical angle and cervical length in early and mid-pregnancy and their value in predicting spontaneous preterm birth
Abstract
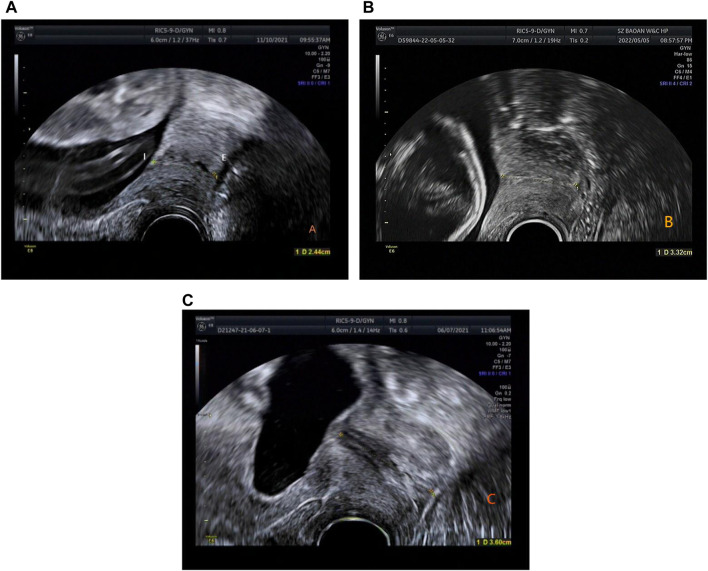
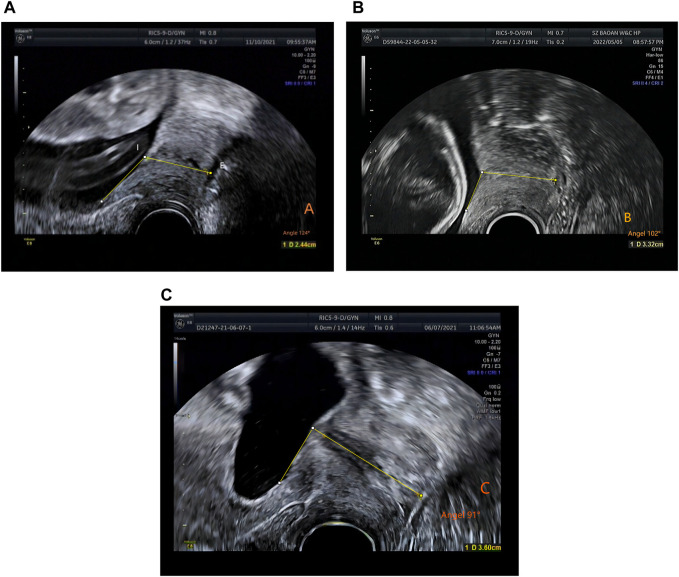
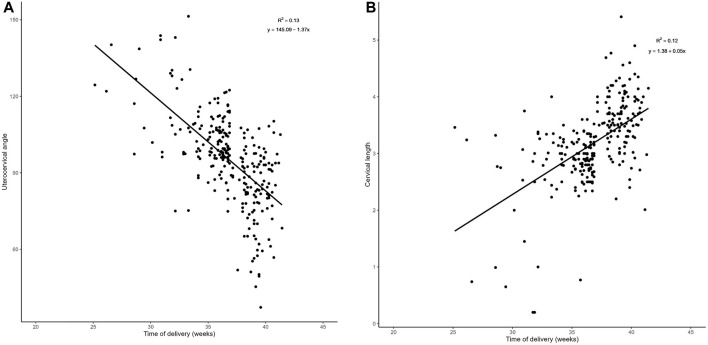
Objective: To explore the feasibility of transvaginal ultrasound measurement of uterocervical angle (UCA) and cervical length (CL) in early and mid-pregnancy and evaluate their combined prediction of spontaneous preterm birth (sPTB) in singleton pregnancies. Patients and Methods: This retrospective study comprised 274 pregnant women who underwent transvaginal ultrasound measurement of CL in mid-pregnancy (15-23+6 weeks); in 75 among them, CL also had been measured in early-pregnancy (<14 weeks). These 274 pregnant women were further divided into a preterm group (n = 149, <37 weeks gestation) and a control group (n = 125, >37 weeks gestation) according to delivery before or after 37 weeks, respectively. In the preterm group, 35 patients delivered before 34 weeks and the remaining 114 delivered between 34 and 37 weeks. Results: The optimal threshold of CL to predict preterm birth risk in women with <37 weeks gestation was 3.38 cm, and the optimal threshold of the UCA to predict preterm birth risk in the same group of women was 96°. The optimal threshold of CL to predict preterm birth risk in women with <34 weeks gestation was 2.54 cm, while that of the UCA in the same group of patients was 106°. The area under the curve for predicting preterm birth by combining the UCA and CL measurements was greater than that by using the UCA or CL alone (p < 0.01). The sensitivity and specificity for predicting preterm birth at <34 weeks gestation was 71.7% and 86.4%, respectively; and the sensitivity and specificity for predicting preterm birth at <37 weeks gestation was 87.6% and 80.6%, respectively. The difference between the two groups in CL and UCA were not significant in early pregnancy (p > 0.01), but only in mid-pregnancy (p < 0.01). There was a negative correlation between UCA and gestational week at delivery (r = -0.361, p < 0.001) and a positive correlation between CL and gestational week at delivery (r = 0.346, p < 0.001) in mid-pregnancy. The proportion of deliveries at <34 weeks was highest when the UCA was >105°, and the proportion of deliveries between 35 and 37 weeks was highest when the UCA was between 95° and 105°. The proportion of deliveries at <34 weeks was highest when the CL was <2.5 cm. Conclusion: The combination of UCA and CL has a better ability to predict preterm birth than either measurement alone. A more obtuse UCA or a shorter CL is associated with an earlier spontaneous preterm birth. The UCA increases from early to mid-pregnancy, while the CL decreases from early to mid-pregnancy.
Keywords: cervical length; early and mid-pregnancy; spontaneous preterm birth; transvaginal ultrasound examination; uterocervical angle.
Copyright © 2024 Zhang, Li, Tian, Li, Zhang and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Distribution of uterocervical angles of pregnant women at 16+ 0 to 23+ 6 weeks gestation with low risk for preterm birth: first vietnamese cohort of women with singleton pregnancies.BMC Pregnancy Childbirth. 2023 Apr 28;23(1):301. doi: 10.1186/s12884-023-05597-3. BMC Pregnancy Childbirth. 2023. PMID: 37118695 Free PMC article.
-
Evaluation of Uterocervical Angle and Cervical Length as Predictors of Spontaneous Preterm Birth.Indian J Radiol Imaging. 2022 Feb 28;32(1):10-15. doi: 10.1055/s-0041-1741411. eCollection 2022 Mar. Indian J Radiol Imaging. 2022. PMID: 35722650 Free PMC article.
-
Uterocervical angle measurement for preterm birth prediction in singleton pregnant women with no history of preterm birth and normal cervical length: A prospective cohort study.Eur J Obstet Gynecol Reprod Biol. 2020 Sep;252:30-35. doi: 10.1016/j.ejogrb.2020.06.020. Epub 2020 Jun 9. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 32562939
-
Utero-cervical angle to predict the risk of spontaneous preterm birth: a review of literature.Minerva Obstet Gynecol. 2024 Aug;76(4):370-375. doi: 10.23736/S2724-606X.24.05433-2. Epub 2024 May 21. Minerva Obstet Gynecol. 2024. PMID: 38771167
-
Uterocervical angle in predicting spontaneous preterm birth: a systematic review and meta-analysis.AJOG Glob Rep. 2023 Jun 12;3(3):100240. doi: 10.1016/j.xagr.2023.100240. eCollection 2023 Aug. AJOG Glob Rep. 2023. PMID: 37396342 Free PMC article. Review.
Cited by
-
Establishment and validation of a prognostic model for premature rupture of membranes and preterm delivery in pregnant women after cervical conization.Am J Transl Res. 2024 Oct 15;16(10):5923-5932. doi: 10.62347/VNQF3805. eCollection 2024. Am J Transl Res. 2024. PMID: 39544738 Free PMC article.
-
Cervical sliding sign and cervical funneling in the third trimester as predictors of spontaneous preterm birth in singleton pregnancy.Quant Imaging Med Surg. 2025 Jul 1;15(7):6005-6015. doi: 10.21037/qims-24-2439. Epub 2025 Jun 30. Quant Imaging Med Surg. 2025. PMID: 40727373 Free PMC article.
References
-
- Blencowe H., Cousens S., Oestergaard M. Z., Chou D., Moller A. B., Narwal R., et al. (2012). National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 379, 2162–2172. 10.1016/S0140-6736(12)60820-4 - DOI - PubMed
-
- Cunningham F. G., Leveno K. G., Bloom S. L., Spong C. Y. (2014). “Preterm labor,” in William obstetrics, twenty-fourth. Editors Cunningham F., Leveno K. G., Bloom S. L., Spong C. Y. (New York: McGraw-Hill Education/Medical; ), 829–830.
LinkOut - more resources
Full Text Sources