

Musculoskeletal disorders in padel: from biomechanics to sonography
- PMID: 38578364
- PMCID: PMC11178742
- DOI: 10.1007/s40477-023-00869-2
Musculoskeletal disorders in padel: from biomechanics to sonography
Abstract
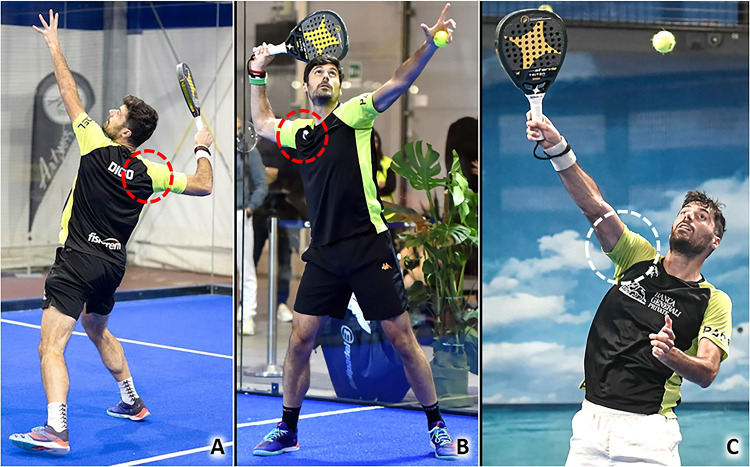
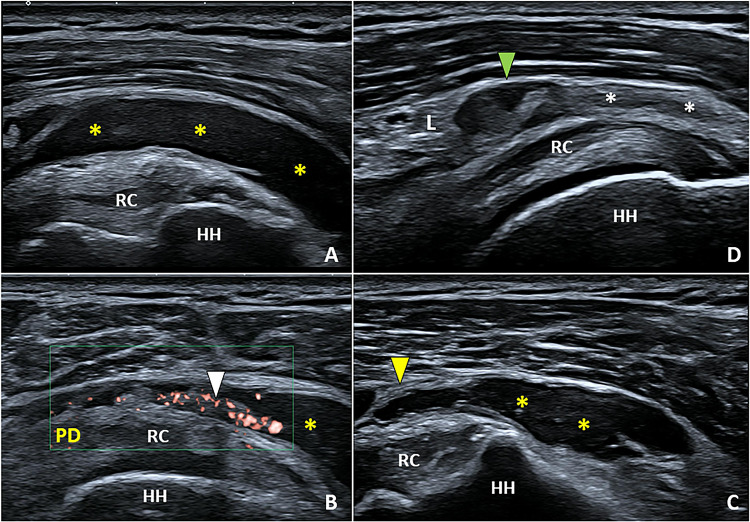
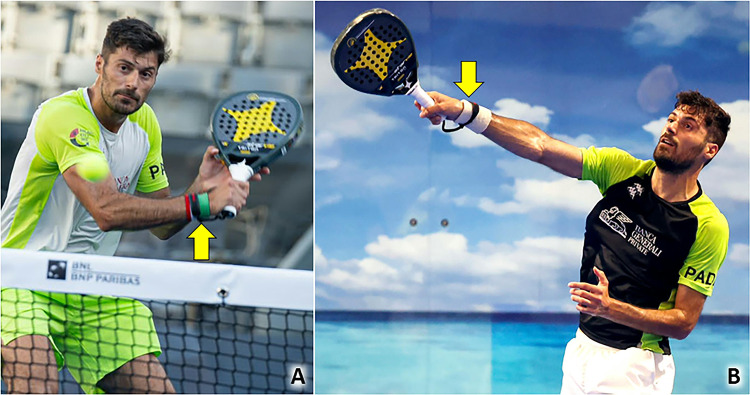
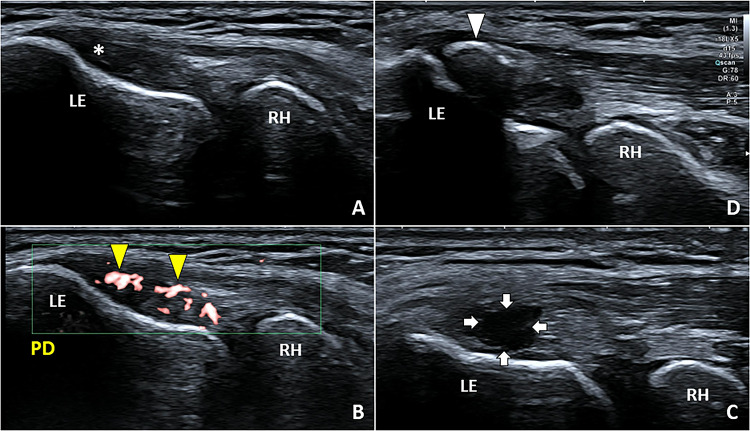
Padel is a racket sport, combining high-frequency and low-intensity athletic gestures, that has been gaining growing scientific interest in recent years. Musculoskeletal injuries are very common among padel players with an incidence rate of 3 per 1000 h of training and 8 per 1000 matches. To the best of our knowledge, a comprehensive collection describing the most common sonographic findings in padel players with musculoskeletal injuries is lacking in the pertinent literature. In this sense, starting from the biomechanical features of padel-specific gestures we have reported the ultrasonographic patterns of most frequent injuries involving the upper limb, the trunk, and the lower limb. Indeed, comprehensive knowledge of the biomechanical and clinical features of musculoskeletal injuries in padel is paramount to accurately perform a detailed ultrasound examination of the affected anatomical site. So, the present investigation aims to provide a practical guide, simple and ready-to-use in daily practice, to optimize the sonographic assessment of padel players by combining it with the clinical findings and the biomechanical features of athletic gestures.
Keywords: Biomechanics; Injuries; Musculoskeletal; Padel; Ultrasound.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
