

Development of a Health Behavioral Digital Intervention for Patients With Hypertension Based on an Intelligent Health Promotion System and WeChat: Randomized Controlled Trial
- PMID: 38578692
- PMCID: PMC11031705
- DOI: 10.2196/53006
Development of a Health Behavioral Digital Intervention for Patients With Hypertension Based on an Intelligent Health Promotion System and WeChat: Randomized Controlled Trial
Abstract
Background: The effectiveness of timely medication, physical activity (PA), a healthy diet, and blood pressure (BP) monitoring for promoting health outcomes and behavioral changes among patients with hypertension is supported by a substantial amount of literature, with "adherence" playing a pivotal role. Nevertheless, there is a lack of consistent evidence regarding whether digital interventions can improve adherence to healthy behaviors among individuals with hypertension.
Objective: The aim was to develop a health behavioral digital intervention for hypertensive patients (HBDIHP) based on an intelligent health promotion system and WeChat following the behavior change wheel (BCW) theory and digital micro-intervention care (DMIC) model and assess its efficacy in controlling BP and improving healthy behavior adherence.
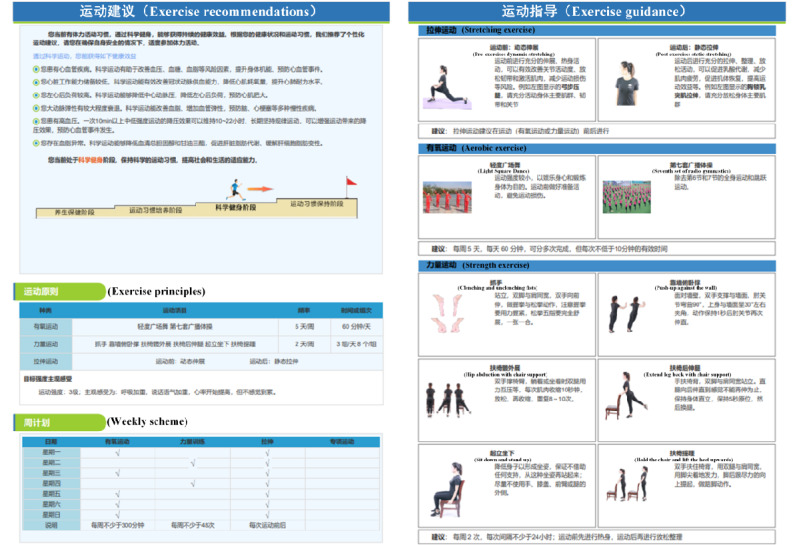
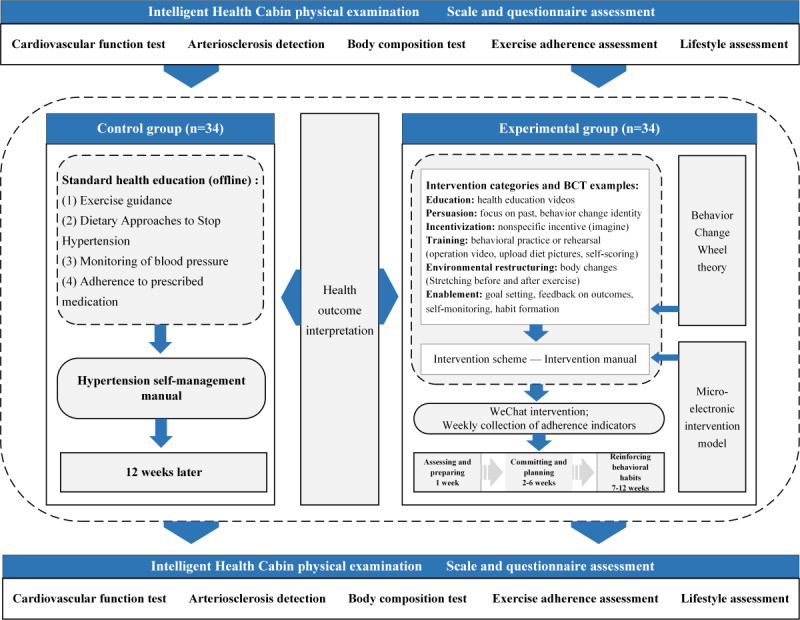
Methods: A 2-arm, randomized trial design was used. We randomly assigned 68 individuals aged >60 years with hypertension in a 1:1 ratio to either the control or experimental group. The digital intervention was established through the following steps: (1) developing digital health education materials focused on adherence to exercise prescriptions, Dietary Approaches to Stop Hypertension (DASH), prescribed medication, and monitoring of BP; (2) using the BCW theory to select behavior change techniques; (3) constructing the intervention's logic following the guidelines of the DMIC model; (4) creating an intervention manual including the aforementioned elements. Prior to the experiment, participants underwent physical examinations at the community health service center's intelligent health cabin and received intelligent personalized health recommendations. The experimental group underwent a 12-week behavior intervention via WeChat, while the control group received routine health education and a self-management manual. The primary outcomes included BP and adherence indicators. Data analysis was performed using SPSS, with independent sample t tests, chi-square tests, paired t tests, and McNemar tests. A P value <.05 was considered statistically significant.
Results: The final analysis included 54 participants with a mean age of 67.24 (SD 4.19) years (n=23 experimental group, n=31 control group). The experimental group had improvements in systolic BP (-7.36 mm Hg, P=.002), exercise time (856.35 metabolic equivalent [MET]-min/week, P<.001), medication adherence (0.56, P=.001), BP monitoring frequency (P=.02), and learning performance (3.23, P<.001). Both groups experienced weight reduction (experimental: 1.2 kg, P=.002; control: 1.11 kg, P=.009) after the intervention. The diet types and quantities for both groups (P<.001) as well as the subendocardial viability ratio (0.16, P=.01) showed significant improvement. However, there were no statistically significant changes in other health outcomes.
Conclusions: The observations suggest our program may have enhanced specific health outcomes and adherence to health behaviors in older adults with hypertension. However, a longer-term, larger-scale trial is necessary to validate the effectiveness.
Trial registration: Chinese Clinical Trial Registry ChiCTR2200062643; https://www.chictr.org.cn/showprojEN.html?proj=172782.
International registered report identifier (irrid): RR2-10.2196/46883.
Keywords: adherence; digital health; health behavior; hypertension; mHealth.
©Ting Sun, Xuejie Xu, Zenghui Ding, Hui Xie, Linlin Ma, Jing Zhang, Yuxin Xia, Guoli Zhang, Zuchang Ma. Originally published in JMIR mHealth and uHealth (https://mhealth.jmir.org), 05.04.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures








Similar articles
-
Evaluating a WeChat-Based Health Behavioral Digital Intervention for Patients With Hypertension: Protocol for a Randomized Controlled Trial.JMIR Res Protoc. 2023 Sep 12;12:e46883. doi: 10.2196/46883. JMIR Res Protoc. 2023. PMID: 37698909 Free PMC article.
-
Efficacy of an mHealth App to Support Patients' Self-Management of Hypertension: Randomized Controlled Trial.J Med Internet Res. 2023 Dec 19;25:e43809. doi: 10.2196/43809. J Med Internet Res. 2023. PMID: 38113071 Free PMC article. Clinical Trial.
-
Efficacy of a WeChat-Based Multimodal Digital Transformation Management Model in New-Onset Mild to Moderate Hypertension: Randomized Clinical Trial.J Med Internet Res. 2023 Dec 4;25:e52464. doi: 10.2196/52464. J Med Internet Res. 2023. PMID: 38048156 Free PMC article. Clinical Trial.
-
The Effectiveness of Self-Management of Hypertension in Adults Using Mobile Health: Systematic Review and Meta-Analysis.JMIR Mhealth Uhealth. 2020 Mar 27;8(3):e17776. doi: 10.2196/17776. JMIR Mhealth Uhealth. 2020. PMID: 32217503 Free PMC article.
-
Effectiveness of digital health interventions on blood pressure control, lifestyle behaviours and adherence to medication in patients with hypertension in low-income and middle-income countries: a systematic review and meta-analysis of randomised controlled trials.EClinicalMedicine. 2024 Feb 1;69:102432. doi: 10.1016/j.eclinm.2024.102432. eCollection 2024 Mar. EClinicalMedicine. 2024. PMID: 38333367 Free PMC article. Review.
Cited by
-
Effectiveness of nursing intervention session on health locus of control and self efficacy for women with preeclampsia.BMC Pregnancy Childbirth. 2025 Apr 23;25(1):468. doi: 10.1186/s12884-025-07447-w. BMC Pregnancy Childbirth. 2025. PMID: 40269741 Free PMC article.
-
Systematic review and meta analysis of standalone digital behavior change interventions on physical activity.NPJ Digit Med. 2025 Jul 14;8(1):436. doi: 10.1038/s41746-025-01827-4. NPJ Digit Med. 2025. PMID: 40659761 Free PMC article.
-
Impact of a mobile health intervention on health management among children with phenylketonuria based on a multi-theory model of the behavior change wheel theory and family health theory: protocol for a randomized controlled trial.Front Psychiatry. 2025 May 27;16:1583804. doi: 10.3389/fpsyt.2025.1583804. eCollection 2025. Front Psychiatry. 2025. PMID: 40496820 Free PMC article.
-
The development and application of the mobile frailty management platform for Chinese community-dwelling older adults.Int J Nurs Sci. 2025 Feb 14;12(2):115-122. doi: 10.1016/j.ijnss.2025.02.005. eCollection 2025 Mar. Int J Nurs Sci. 2025. PMID: 40241871 Free PMC article.
-
Effects of a health education intervention based on the behavior change wheel on fear of hypoglycemia behavior in type 2 diabetes mellitus patients: a randomized controlled pilot trial.Acta Diabetol. 2025 Jun 23. doi: 10.1007/s00592-025-02549-5. Online ahead of print. Acta Diabetol. 2025. PMID: 40548996
References
-
- NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021 Sep 11;398(10304):957–980. doi: 10.1016/S0140-6736(21)01330-1. http://hdl.handle.net/2318/1805296 S0140-6736(21)01330-1 - DOI - PMC - PubMed
-
- Wu J, Napoleone J, Linke S, Noble M, Turken M, Rakotz M, Kirley K, Folk Akers J, Juusola J, Jasik CB. Long-term results of a digital hypertension self-management program: retrospective cohort study. JMIR Cardio. 2023 Aug 24;7:e43489. doi: 10.2196/43489. https://cardio.jmir.org/2023//e43489/ v7i1e43489 - DOI - PMC - PubMed
-
- Edwards JJ, Deenmamode AHP, Griffiths M, Arnold O, Cooper NJ, Wiles JD, O'Driscoll JM. Exercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trials. Br J Sports Med. 2023 Oct;57(20):1317–1326. doi: 10.1136/bjsports-2022-106503.bjsports-2022-106503 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
