

The epidemiology of invasive fungal infections in transplant recipients
- PMID: 38580051
- PMCID: PMC11220536
- DOI: 10.1016/j.bj.2024.100719
The epidemiology of invasive fungal infections in transplant recipients
Abstract
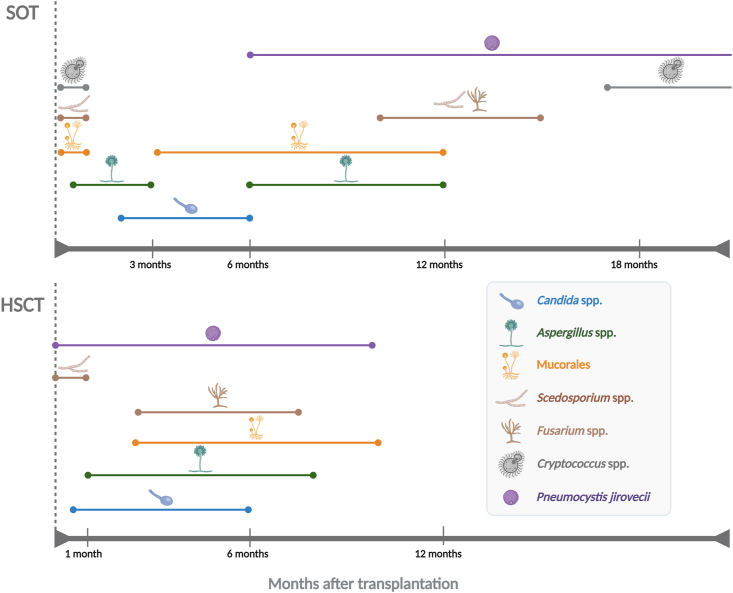
Transplant patients, including solid-organ transplant (SOT) and hematopoietic stem cell transplant (HSCT) recipients, are exposed to various types of complications, particularly rejection. To prevent these outcomes, transplant recipients commonly receive long-term immunosuppressive regimens that in turn make them more susceptible to a wide array of infectious diseases, notably those caused by opportunistic pathogens. Among these, invasive fungal infections (IFIs) remain a major cause of mortality and morbidity in both SOT and HSCT recipients. Despite the continuing improvement in early diagnostics and treatments of IFIs, the management of these infections in transplant patients is still complicated. Here, we provide an overview concerning the most recent trends in the epidemiology of IFIs in SOT and HSCT recipients by describing the prominent yeast and mold species involved, the timing of post-transplant IFIs and the risk factors associated with their occurrence in these particularly weak populations. We also give special emphasis into basic research advances in the field that recently suggested a role of the global and long-term prophylactic regimen in orchestrating various biological disturbances in the organism and conditioning the emergence of the most adapted fungal strains to the particular physiological profiles of transplant patients.
© 2024 The Authors. Published by Elsevier B.V. on behalf of Chang Gung University. This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/).
Figures


References
-
- Desoubeaux G, Chesnay A. Health threat caused by fungi of medical interest: where are we in 2021? Front Biosci. 2021;26(9):409. 12. - PubMed
-
- Jenks JD, Cornely OA, Chen SCA, Thompson GR, Hoenigl M. Breakthrough invasive fungal infections: who is at risk? Mycoses. 2020;63(10):1021. 32. - PubMed
-
- World Health Organization . Transplantation. 2022. https://www.who.int/transplantation/gkt/statistics/en/ Accessed.
-
- Pappas PG, Alexander BD, Andes DR, Hadley S, Kauffman CA, Freifeld A, et al. Invasive fungal infections among organ transplant recipients: results of the Transplant-Associated Infection Surveillance Network (TRANSNET) Clin Infect Dis. 2010;50(8):1101. 11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
