

Combining CRISPR-Cas9 and TCR exchange to generate a safe and efficient cord blood-derived T cell product for pediatric relapsed AML
- PMID: 38580329
- PMCID: PMC11002379
- DOI: 10.1136/jitc-2023-008174
Combining CRISPR-Cas9 and TCR exchange to generate a safe and efficient cord blood-derived T cell product for pediatric relapsed AML
Abstract
Background: Hematopoietic cell transplantation (HCT) is an effective treatment for pediatric patients with high-risk, refractory, or relapsed acute myeloid leukemia (AML). However, a large proportion of transplanted patients eventually die due to relapse. To improve overall survival, we propose a combined strategy based on cord blood (CB)-HCT with the application of AML-specific T cell receptor (TCR)-engineered T cell therapy derived from the same CB graft.
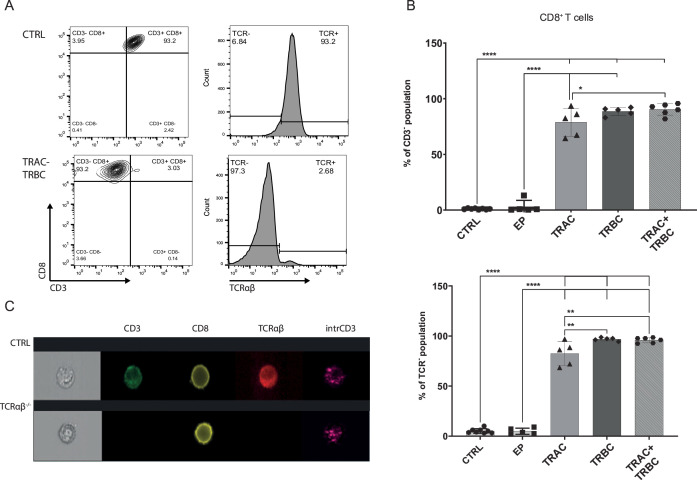
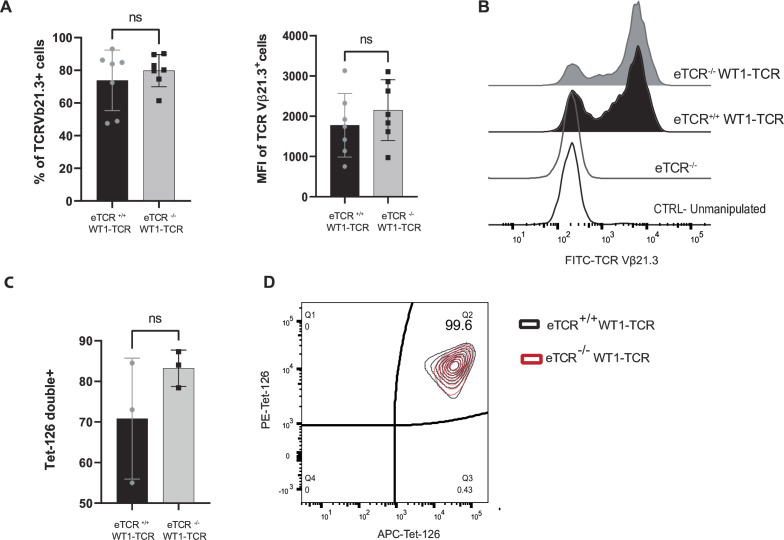
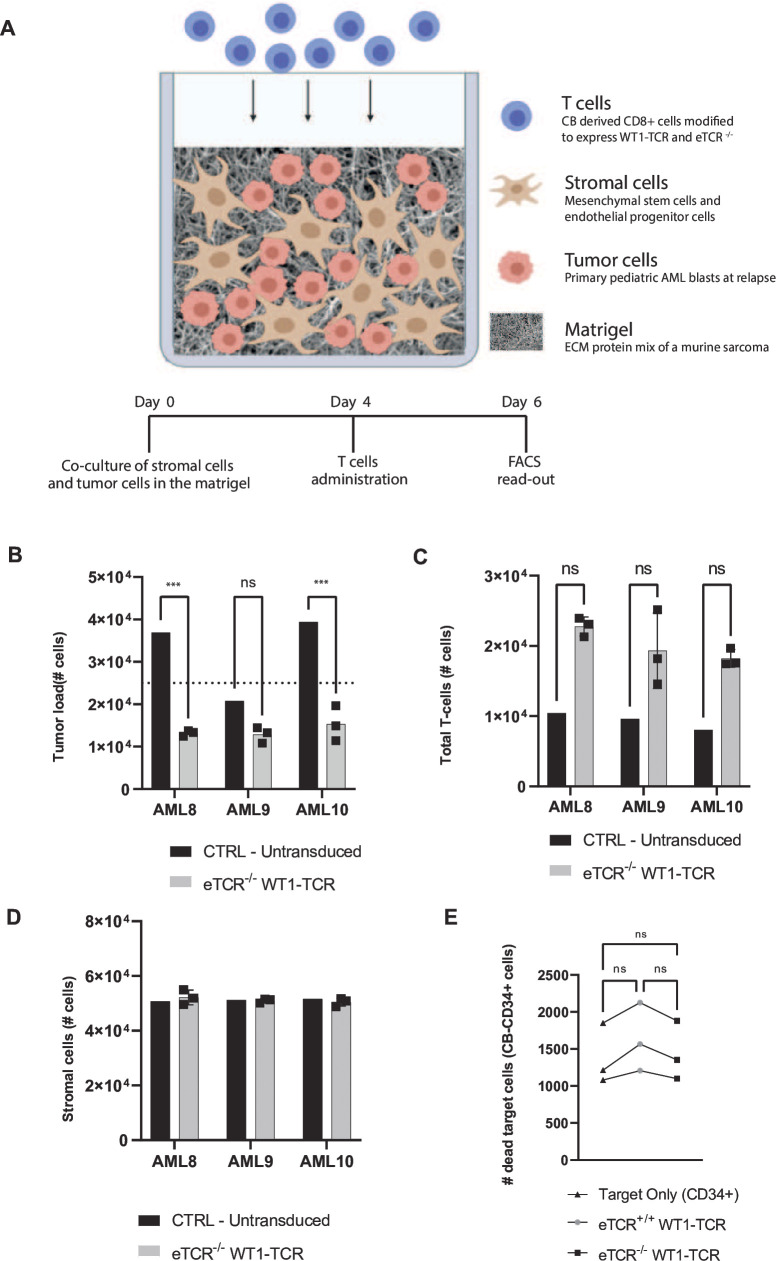
Methods: We produced CB-CD8+ T cells expressing a recombinant TCR (rTCR) against Wilms tumor 1 (WT1) while lacking endogenous TCR (eTCR) expression to avoid mispairing and competition. CRISPR-Cas9 multiplexing was used to target the constant region of the endogenous TCRα (TRAC) and TCRβ (TRBC) chains. Next, an optimized method for lentiviral transduction was used to introduce recombinant WT1-TCR. The cytotoxic and migration capacity of the product was evaluated in coculture assays for both cell lines and primary pediatric AML blasts.
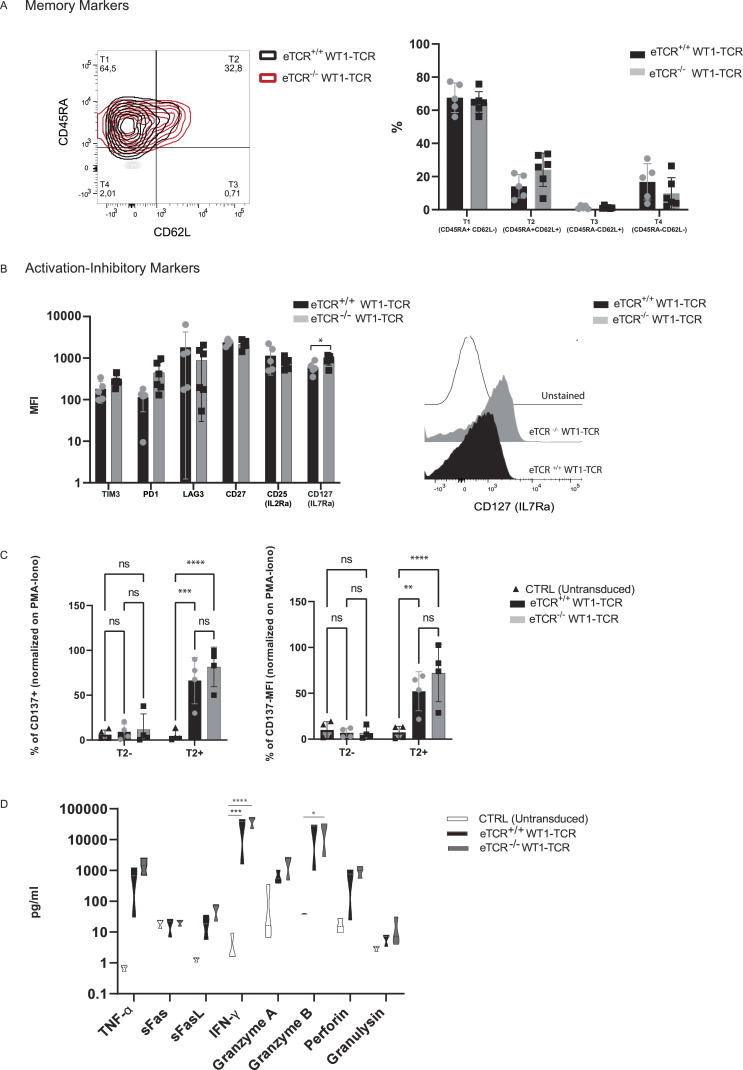
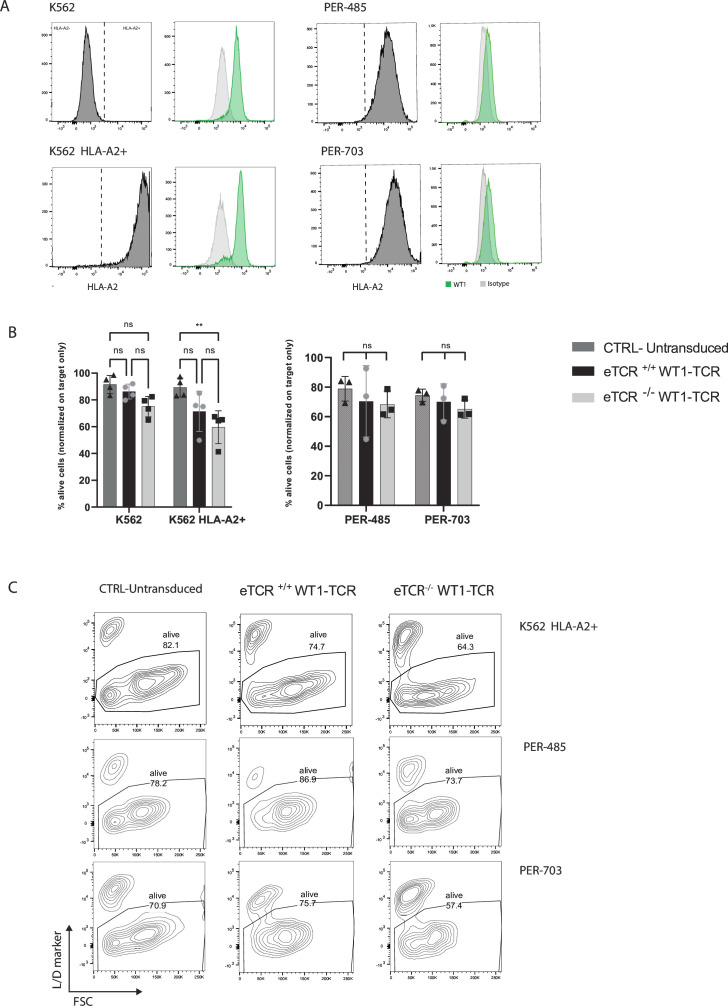
Results: The gene editing and transduction procedures achieved high efficiency, with up to 95% of cells lacking eTCR and over 70% of T cells expressing rWT1-TCR. WT1-TCR-engineered T cells lacking the expression of their eTCR (eTCR-/- WT1-TCR) showed increased cell surface expression of the rTCR and production of cytotoxic cytokines, such as granzyme A and B, perforin, interferon-γ (IFNγ), and tumor necrosis factor-α (TNFα), on antigen recognition when compared with WT1-TCR-engineered T cells still expressing their eTCR (eTCR+/+ WT1-TCR). CRISPR-Cas9 editing did not affect immunophenotypic characteristics or T cell activation and did not induce increased expression of inhibitory molecules. eTCR-/- WT1-TCR CD8+ CB-T cells showed effective migratory and killing capacity in cocultures with neoplastic cell lines and primary AML blasts, but did not show toxicity toward healthy cells.
Conclusions: In summary, we show the feasibility of developing a potent CB-derived CD8+ T cell product targeting WT1, providing an option for post-transplant allogeneic immune cell therapy or as an off-the-shelf product, to prevent relapse and improve the clinical outcome of children with AML.
Keywords: CD8-Positive T-Lymphocytes; Cell Engineering; Hematologic Neoplasms; Pediatrics; T cell Receptor - TCR.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JK reports grants from Gadeta, Novartis, and Miltenyi Biotec and is the inventor of patents dealing with γδT cell-related aspects, as well as the cofounder and shareholder of Gadeta. ZS is an inventor of patents dealing with γδT cell-related aspects.
Figures
References
-
- Rasche M, Zimmermann M, Borschel L, et al. . Successes and challenges in the treatment of pediatric acute myeloid leukemia: a retrospective analysis of the AML-BFM trials from 1987 to 2012. Leukemia 2018;32:2167–77. 10.1038/s41375-018-0071-7 Available: 10.1038/s41375-018-0071-7 - DOI - DOI - PMC - PubMed
-
- Bergmann L, Miething C, Maurer U, et al. . High levels of Wilms' tumor gene (Wt1) mRNA in acute myeloid leukemias are associated with a worse long-term outcome. Blood 1997;90:1217–25. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials