

Predicting adverse events after thoracic endovascular aortic repair for patients with type B aortic dissection
- PMID: 38580650
- PMCID: PMC10997599
- DOI: 10.1038/s41598-024-58106-7
Predicting adverse events after thoracic endovascular aortic repair for patients with type B aortic dissection
Abstract
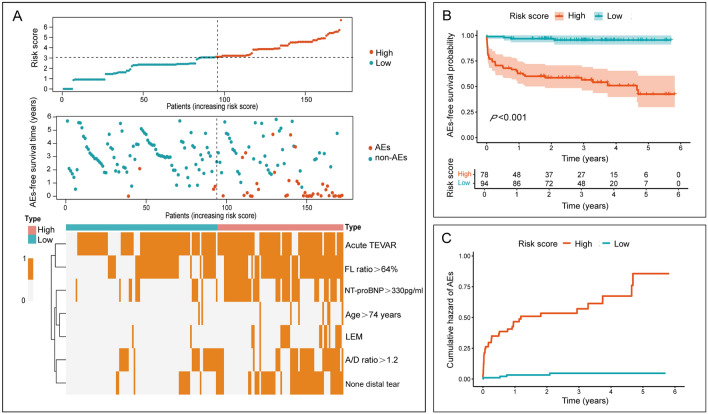
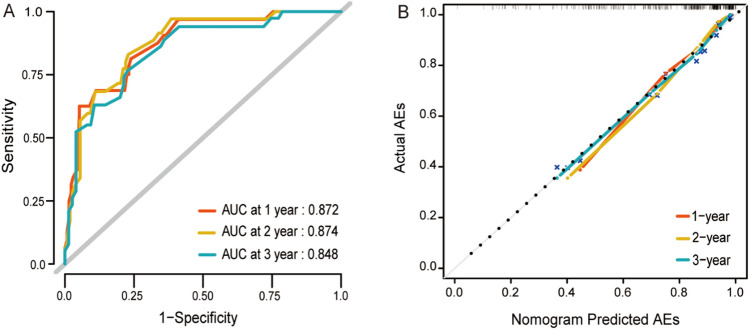
The potential of adverse events (AEs) after thoracic endovascular aortic repair (TEVAR) in patients with type B aortic dissection (TBAD) has been reported. To avoid the occurrence of AEs, it is important to recognize high-risk population for prevention in advance. The data of 261 patients with TBAD who received TEVAR between June 2017 and June 2021 at our medical center were retrospectively reviewed. After the implementation of exclusion criteria, 172 patients were finally included, and after 2.8 years (range from 1 day to 5.8 years) of follow up, they were divided into AEs (n = 41) and non-AEs (n = 131) groups. We identified the predictors of AEs, and a prediction model was constructed to calculate the specific risk of postoperative AEs at 1, 2, and 3 years, and to stratify patients into high-risk (n = 78) and low-risk (n = 94) group. The prediction model included seven predictors: Age > 75 years, Lower extremity malperfusion (LEM), NT-proBNP > 330 pg/ml, None distal tear, the ratio between the diameter of the ascending aorta and descending aorta (A/D ratio) > 1.2, the ratio of the area of the false lumen to the total aorta (FL ratio) > 64%, and acute TEVAR, which exhibited excellent predictive accuracy performance and discriminatory ability with C statistic of 82.3% (95% CI 77.3-89.2%). The prediction model was contributed to identify high-risk patients of postoperative AEs, which may serve to achievement of personalized treatment and follow-up plans for patients.
Keywords: Adverse events; Computed tomography angiography; Prediction model; Thoracic endovascular aortic repair; Type B aortic dissection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Implications of secondary aortic intervention after thoracic endovascular aortic repair for acute and chronic type B dissection.J Vasc Surg. 2019 May;69(5):1367-1378. doi: 10.1016/j.jvs.2018.07.080. Epub 2018 Dec 13. J Vasc Surg. 2019. PMID: 30553732 Free PMC article.
-
Impact of proximal seal zone length and intramural hematoma on clinical outcomes and aortic remodeling after thoracic endovascular aortic repair for aortic dissections.J Vasc Surg. 2019 Apr;69(4):987-995. doi: 10.1016/j.jvs.2018.06.219. Epub 2018 Oct 24. J Vasc Surg. 2019. PMID: 30528404
-
Influence of distal extension of false lumen on adverse aortic events after TEVAR in patients with acute type B aortic dissection.Catheter Cardiovasc Interv. 2016 Mar;87 Suppl 1:599-607. doi: 10.1002/ccd.26427. Epub 2016 Feb 10. Catheter Cardiovasc Interv. 2016. PMID: 26864376
-
Fate and Consequences of the False Lumen After Thoracic Endovascular Aortic Repair in Type B Aortic Dissection.Ann Vasc Surg. 2023 Aug;94:32-37. doi: 10.1016/j.avsg.2022.09.042. Epub 2022 Oct 26. Ann Vasc Surg. 2023. PMID: 36309167 Review.
-
Management of left subclavian artery in type B aortic dissection treated with thoracic endovascular aorta repair.J Vasc Surg. 2023 May;77(5):1553-1561.e2. doi: 10.1016/j.jvs.2022.10.013. Epub 2022 Oct 19. J Vasc Surg. 2023. PMID: 36272506 Review.
Cited by
-
Electrokinetic blood flow of Carreau ternary nanofluids in stenotic arteries with thermal reactions under CC heat flux for therapy.Sci Rep. 2025 Aug 11;15(1):29370. doi: 10.1038/s41598-025-14211-9. Sci Rep. 2025. PMID: 40790334 Free PMC article.
References
-
- Isselbacher EM, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022;146(24):e334–e482. doi: 10.1161/CIR0000000000001106. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
