

Diagnostic efficacy of contrast-enhanced gastric ultrasonography in staging gastric cancer: a meta-analysis
- PMID: 38580944
- PMCID: PMC10998428
- DOI: 10.1186/s12885-024-12210-z
Diagnostic efficacy of contrast-enhanced gastric ultrasonography in staging gastric cancer: a meta-analysis
Abstract
Background: As comprehensive surgical management for gastric cancer becomes increasingly specialized and standardized, the precise differentiation between ≤T1 and ≥T2 gastric cancer before endoscopic intervention holds paramount clinical significance.
Objective: To evaluate the diagnostic efficacy of contrast-enhanced gastric ultrasonography in differentiating ≤T1 and ≥T2 gastric cancer.
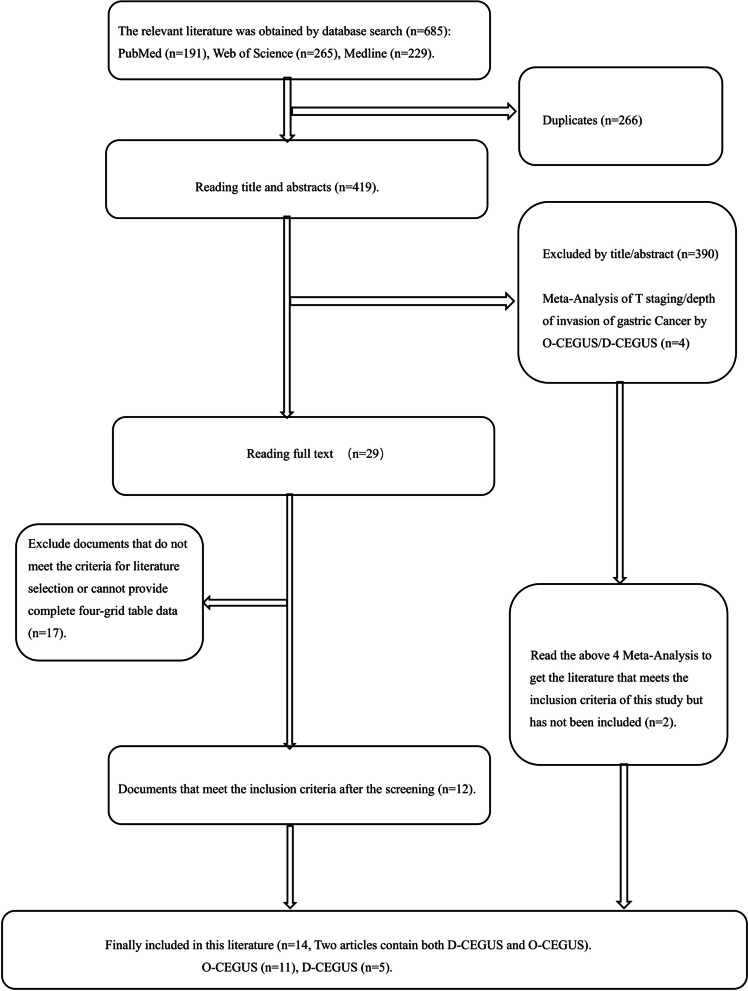
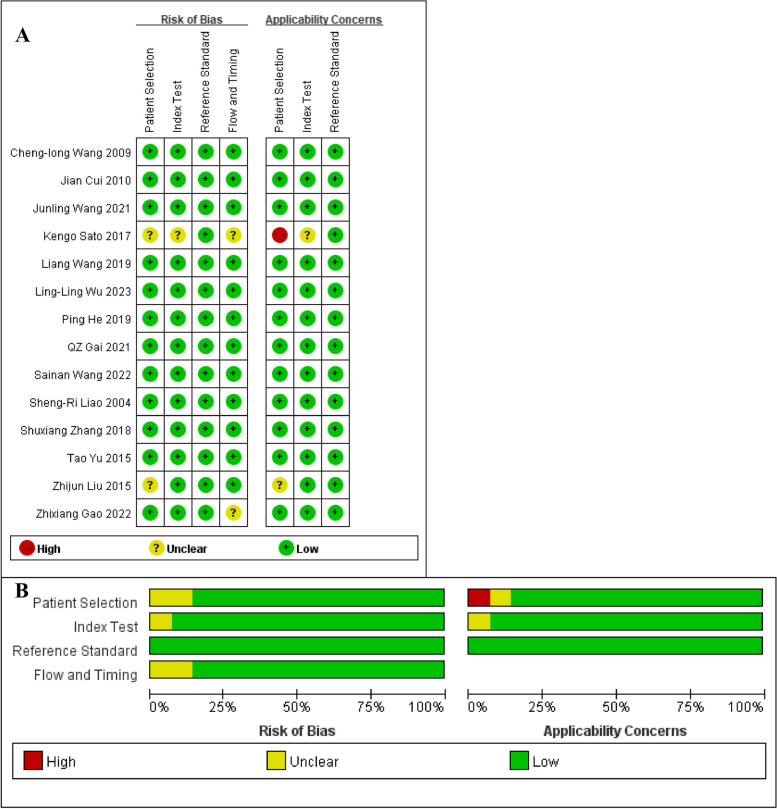
Methods: PubMed, Web of Science, and Medline were searched to collect studies published from January 1, 2000 to March 16, 2023 on the efficacy of either double contrast-enhanced gastric ultrasonography (D-CEGUS) or oral contrast-enhanced gastric ultrasonography (O-CEGUS) in determining T-stage in gastric cancer. The articles were selected according to specified inclusion and exclusion criteria, and the quality of the included literature was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 scale. Meta-analysis was performed using Stata 12 software with data from the 2 × 2 crosslinked tables in the included literature.
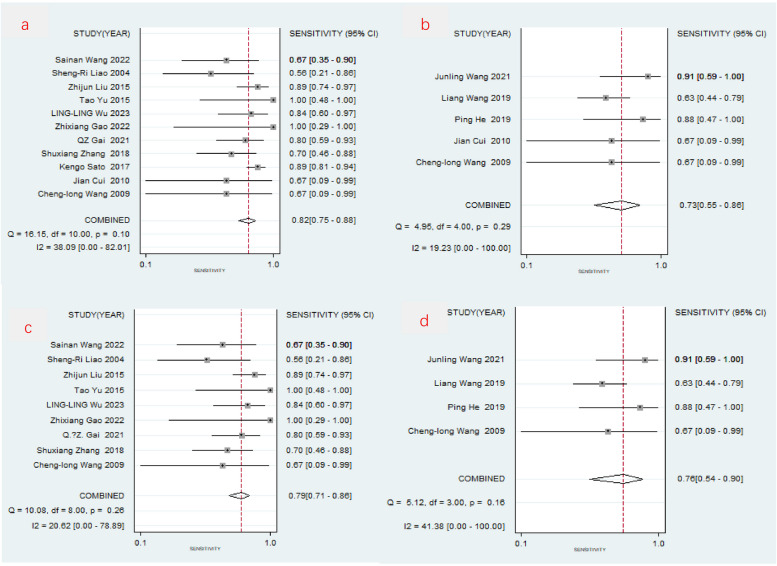
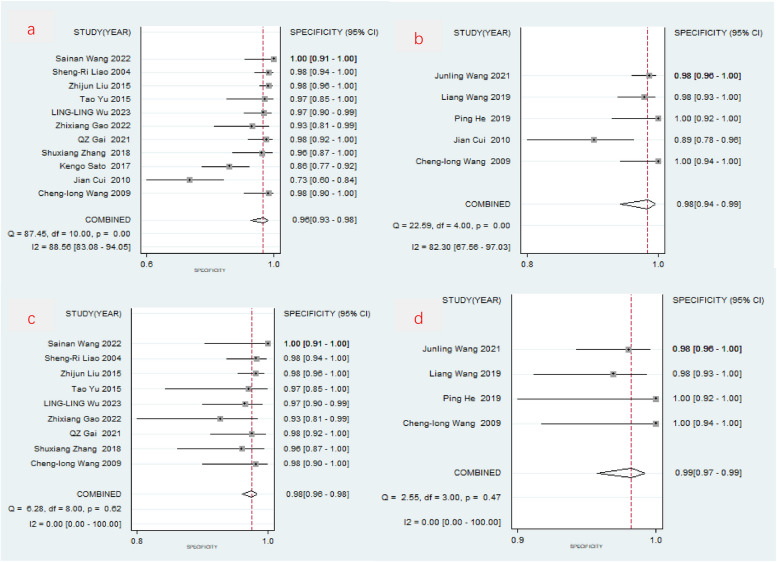
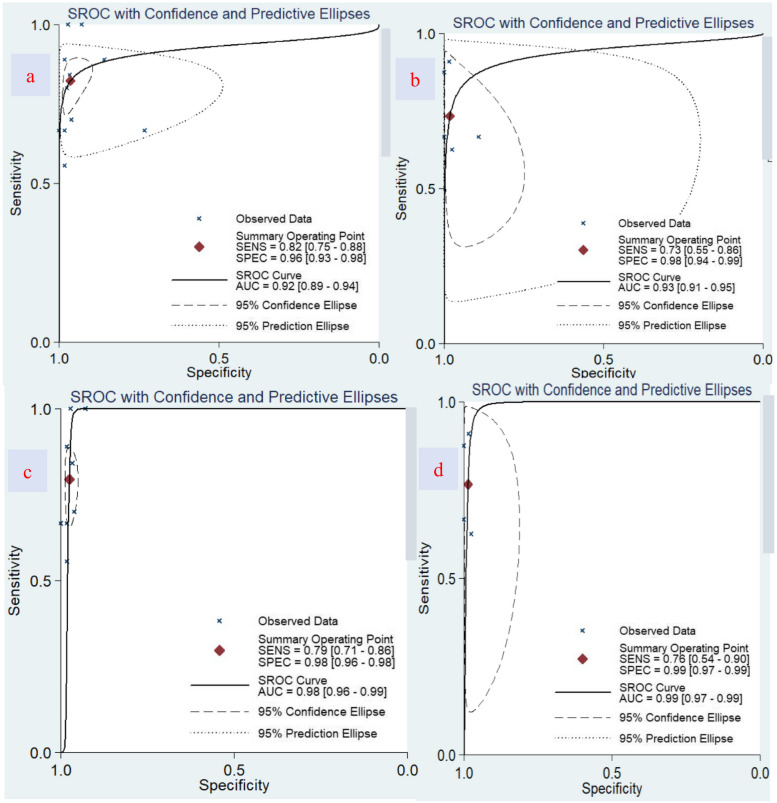
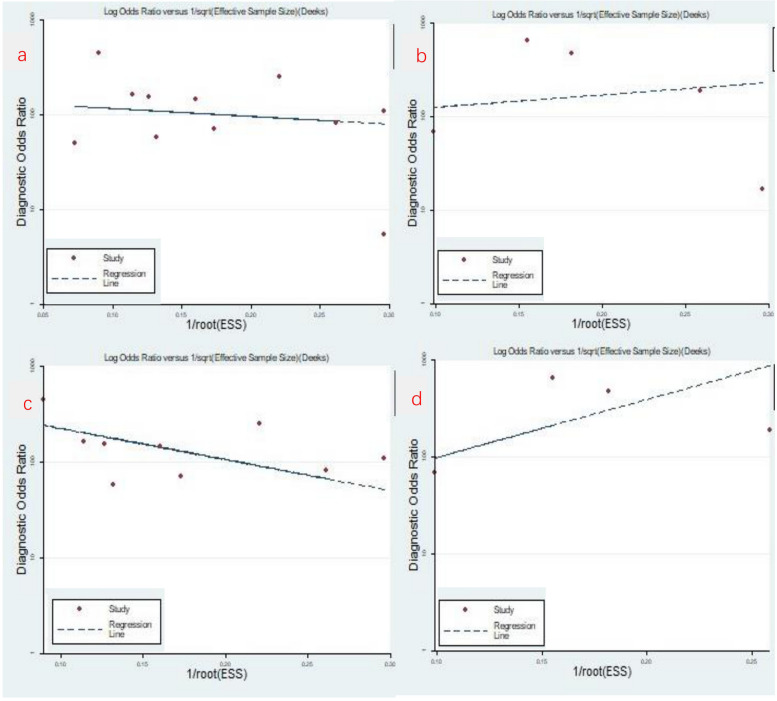
Results: In total, 11 papers with 1124 patients were included in the O-CEGUS analysis, which revealed a combined sensitivity of 0.822 (95% confidence interval [CI] = 0.753-0.875), combined specificity of 0.964 (95% CI = 0.925-0.983), and area under the summary receiver operating characteristic (sROC) curve (AUC) of 0.92 (95% CI = 0.89-0.94). In addition, five studies involving 536 patients were included in the D-CEGUS analysis, which gave a combined sensitivity of 0.733 (95% CI = 0.550-0.860), combined specificity of 0.982 (95% CI = 0.936-0.995), and AUC of 0.93 (95% CI = 0.91-0.95). According to the I2 and P values of the forest plot, there was obvious heterogeneity in the combined specificities of the included papers. Therefore, the two studies with the lowest specificities were excluded from the O-CEGUS and D-CEGUS analyses, which eliminated the heterogeneity among the remaining literature. Consequently, the combined sensitivity and specificity of the remaining studies were 0.794 (95% CI = 0.710-0.859) and 0.976 (95% CI = 0.962-0.985), respectively, for the O-CEDUS studies and 0.765 (95% CI = 0.543-0.899) and 0.986 (95% CI = 0.967-0.994), respectively, for the D-CEGUS studies. The AUCs were 0.98 and 0.99 for O-CEGUS and D-CEGUS studies, respectively.
Conclusion: Both O-CEGUS and D-CEGUS can differentiate ≤T1 gastric cancer from ≥T2 gastric cancer, thus assisting the formulation of clinical treatment strategies for patients with very early gastric cancer. Given its simplicity and cost-effectiveness, O-CEGUS is often favored as a staging method for gastric cancer prior to endoscopic intervention.
Keywords: Contrast agent; Gastric cancer; Gastric ultrasonography; Meta-analysis; T-stage.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Park KB, Jeon CH, Seo HS, Jung YJ, Song KY, Park CH, et al. Operative safety of curative gastrectomy after endoscopic submucosal dissection (ESD) for early gastric cancer - 1:2 propensity score matching analysis: A retrospective single-center study (cohort study) Int J Surg. 2020;80:124–8. doi: 10.1016/j.ijsu.2020.06.041. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
