

Arterial hypertension in infants with congenital diaphragmatic hernia following surgical repair
- PMID: 38581464
- PMCID: PMC11192699
- DOI: 10.1007/s00431-024-05509-3
Arterial hypertension in infants with congenital diaphragmatic hernia following surgical repair
Abstract
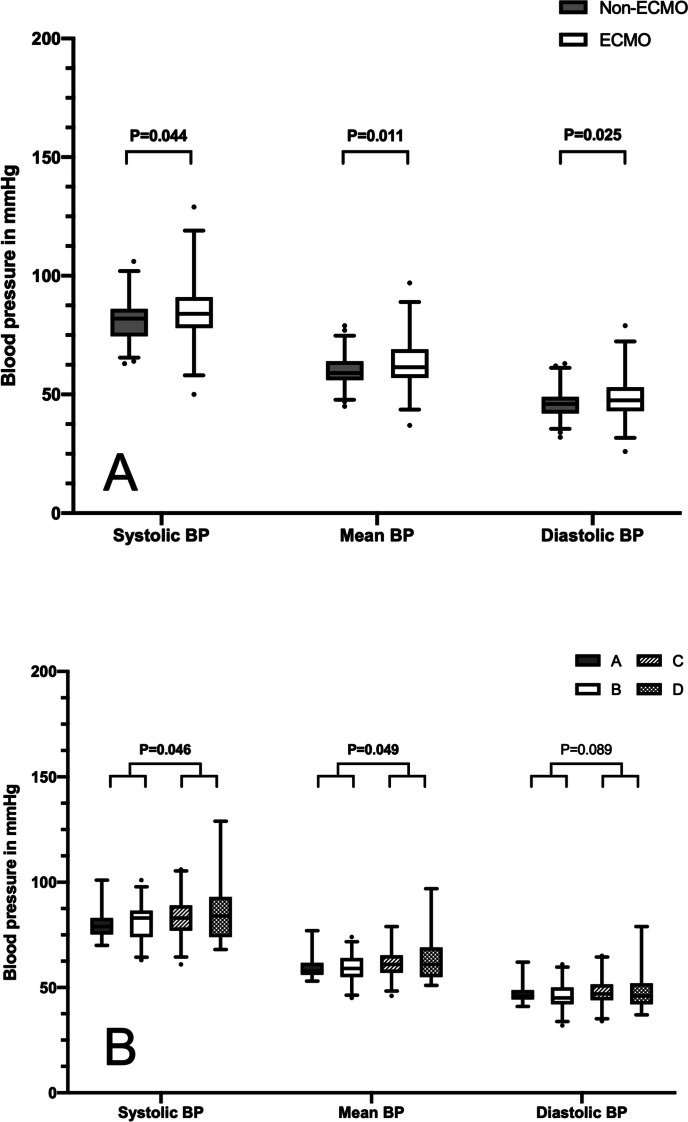
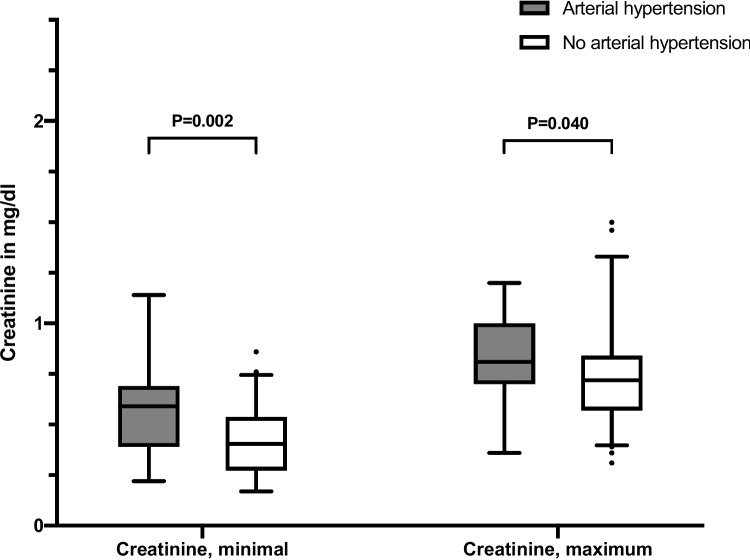
Pulmonary hypertension (PH) and cardiac dysfunction are established comorbidities of congenital diaphragmatic hernia (CDH). However, there is very little data focusing on arterial hypertension in CDH. This study aims to investigate the incidence of arterial hypertension in neonates with CDH at hospital discharge. Archived clinical data of 167 CDH infants who received surgical repair of the diaphragmatic defect and survived for > 60 days were retrospectively analyzed. Blood pressure (BP) values were averaged for the last 7 days before discharge and compared to standard BP values for sex, age, and height provided by the AHA in 2004. BP values reaching or extending the 95th percentile were defined as arterial hypertension. The use of antihypertensive medication was analyzed at discharge and during hospitalization. Arterial hypertension at discharge was observed in 19 of 167 infants (11.3%) of which 12 (63%) were not receiving antihypertensive medication. Eighty patients (47.9%) received antihypertensive medication at any point during hospitalization and 28.9% of 152 survivors (n = 44) received antihypertensive medication at discharge, although in 45.5% (n = 20) of patients receiving antihypertensive medication, the indication for antihypertensive medication was myocardial hypertrophy or frequency control. BP was significantly higher in ECMO compared to non-ECMO patients, despite a similar incidence of arterial hypertension in both groups (13.8% vs. 10.1%, p = 0.473). Non-isolated CDH, formula feeding, and minimal creatinine in the first week of life were significantly associated with arterial hypertension on univariate analysis. Following multivariate analysis, only minimal creatinine remained independently associated with arterial hypertension. Conclusion: This study demonstrates a moderately high incidence of arterial hypertension in CDH infants at discharge and an independent association of creatinine values with arterial hypertension. Physicians should be aware of this risk and include regular BP measurements and test of renal function in CDH care and follow-up. What is Known: • Due to decreasing mortality, morbidity is increasing in surviving CDH patients. • Pulmonary hypertension and cardiac dysfunction are well-known cardiovascular comorbidities of CDH. What is New: • There is a moderately high incidence of arterial hypertension in CDH infants at discharge even in a population with frequent treatment with antihypertensive medication. • A more complicated hospital course (ECMO, higher degree of PH, larger defect size) was associated with a higher risk for arterial hypertension.
Keywords: Arterial hypertension; Blood pressure; Congenital diaphragmatic hernia; Extracorporeal membrane oxygenation; Follow-up.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
