

Identification of cells of leukemic stem cell origin with non-canonical regenerative properties
- PMID: 38582086
- PMCID: PMC11031376
- DOI: 10.1016/j.xcrm.2024.101485
Identification of cells of leukemic stem cell origin with non-canonical regenerative properties
Abstract
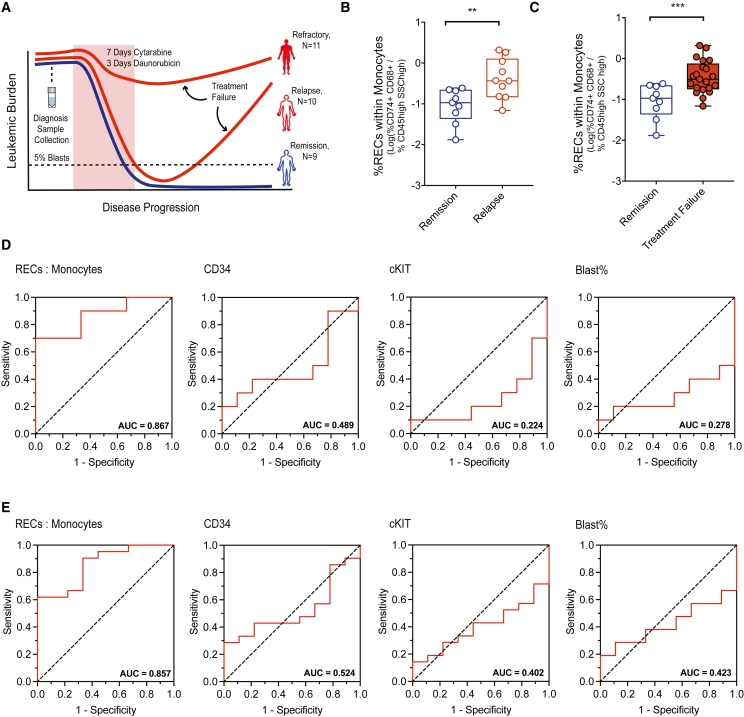
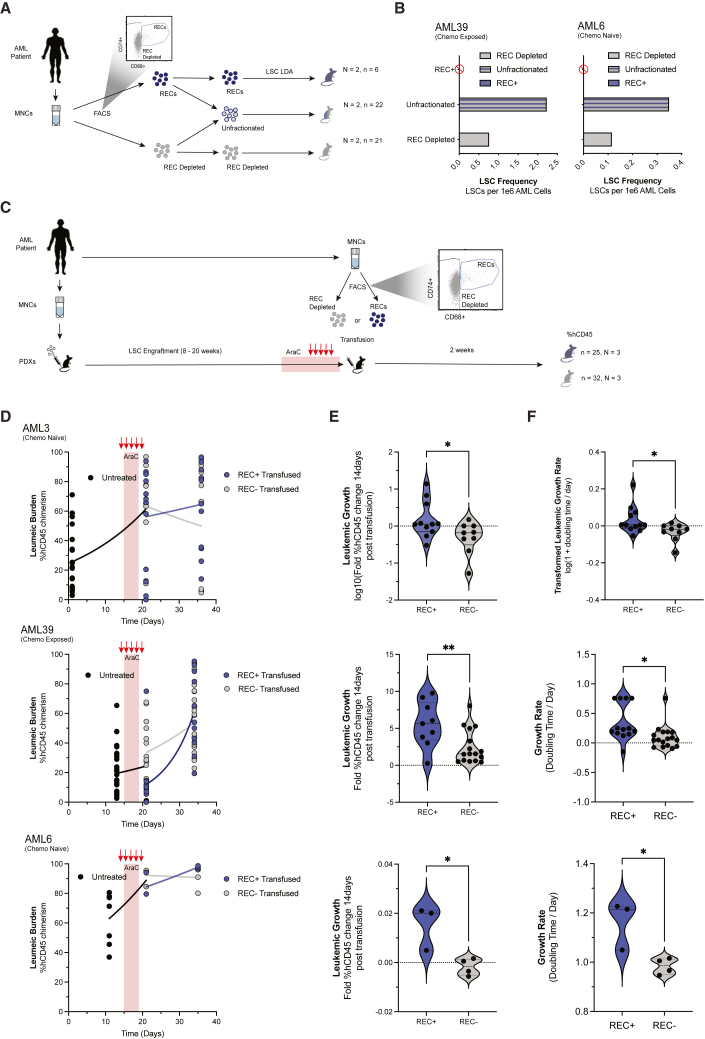
Despite most acute myeloid leukemia (AML) patients entering remission following chemotherapy, outcomes remain poor due to surviving leukemic cells that contribute to relapse. The nature of these enduring cells is poorly understood. Here, through temporal single-cell transcriptomic characterization of AML hierarchical regeneration in response to chemotherapy, we reveal a cell population: AML regeneration enriched cells (RECs). RECs are defined by CD74/CD68 expression, and although derived from leukemic stem cells (LSCs), are devoid of stem/progenitor capacity. Based on REC in situ proximity to CD34-expressing cells identified using spatial transcriptomics on AML patient bone marrow samples, RECs demonstrate the ability to augment or reduce leukemic regeneration in vivo based on transfusion or depletion, respectively. Furthermore, RECs are prognostic for patient survival as well as predictive of treatment failure in AML cohorts. Our study reveals RECs as a previously unknown functional catalyst of LSC-driven regeneration contributing to the non-canonical framework of AML regeneration.
Keywords: Regen71; acute myeloid leukemia; chemotherapy; injury; leukemia stem cells; non-canonical regeneration; regeneration enriched cells; relapse.
Crown Copyright © 2024. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures





References
-
- Döhner H., Estey E., Grimwade D., Amadori S., Appelbaum F.R., Büchner T., Dombret H., Ebert B.L., Fenaux P., Larson R.A., et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129:424–447. doi: 10.1182/blood-2016-08-733196. - DOI - PMC - PubMed
-
- Döhner H., Wei A.H., Appelbaum F.R., Craddock C., DiNardo C.D., Dombret H., Ebert B.L., Fenaux P., Godley L.A., Hasserjian R.P., et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140:1345–1377. doi: 10.1182/blood.2022016867. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
