

Impact of ventricular tachycardia ablation in subcutaneous implantable cardioverter defibrillator carriers: a multicentre, international analysis from the iSUSI project
- PMID: 38584394
- PMCID: PMC10999646
- DOI: 10.1093/europace/euae066
Impact of ventricular tachycardia ablation in subcutaneous implantable cardioverter defibrillator carriers: a multicentre, international analysis from the iSUSI project
Abstract
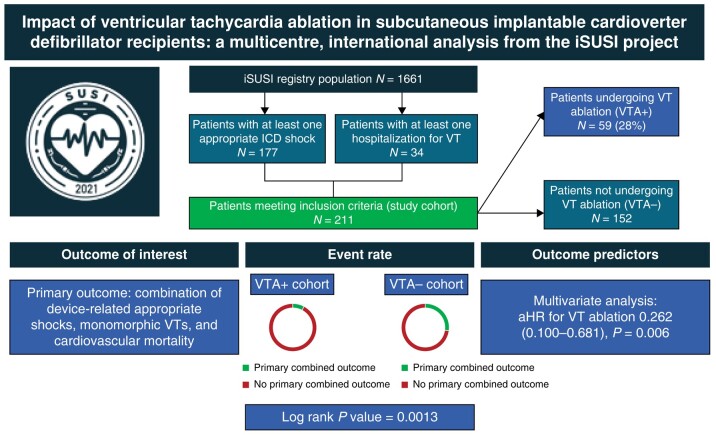
Aims: Catheter ablation (CA) of ventricular tachycardia (VT) has become an important tool to improve clinical outcomes in patients with appropriate transvenous implantable cardioverter defibrillator (ICD) shocks. The aim of our analysis was to test whether VT ablation (VTA) impacts long-term clinical outcomes even in subcutaneous ICD (S-ICD) carriers.
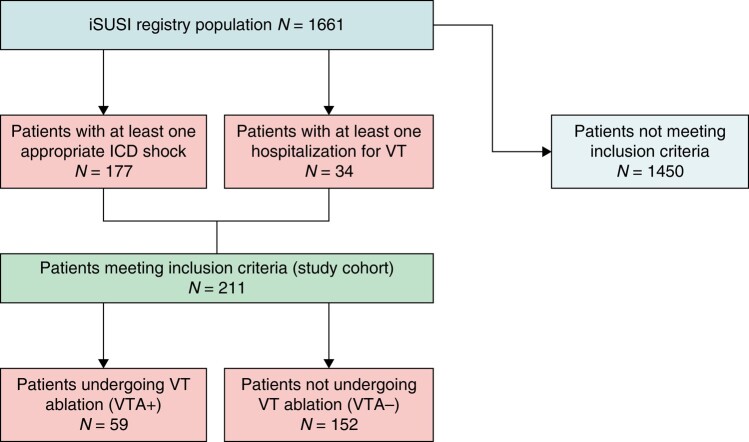
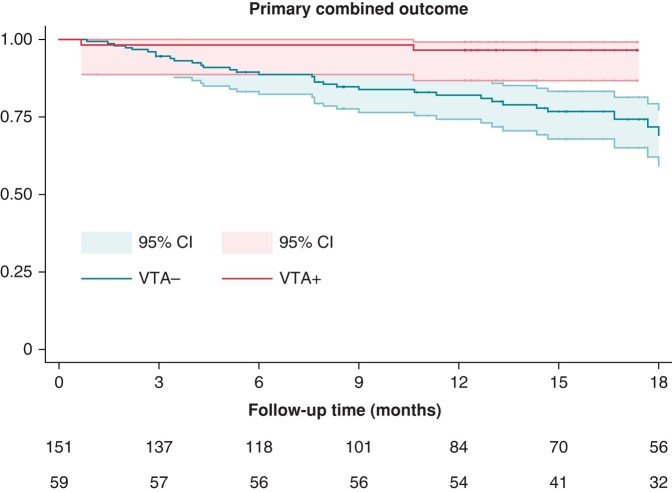
Methods and results: International Subcutaneous Implantable Cardioverter Defibrillator (iSUSI) registry patients who experienced either an ICD shock or a hospitalization for monomorphic VT were included in this analysis. Based on an eventual VTA after the index event, patients were divided into VTA+ vs. VTA- cohorts. Primary outcome of the study was the occurrence of a combination of device-related appropriate shocks, monomorphic VTs, and cardiovascular mortality. Secondary outcomes were addressed individually. Among n = 1661 iSUSI patients, n = 211 were included: n = 177 experiencing ICD shocks and n = 34 hospitalized for VT. No significant differences in baseline characteristics were observed. Both the crude and the yearly event rate of the primary outcome (5/59 and 3.8% yearly event rate VTA+ vs. 41/152 and 16.4% yearly event rate in the VTA-; log-rank: P value = 0.0013) and the cardiovascular mortality (1/59 and 0.7% yearly event rate VTA+ vs. 13/152 and 4.7% yearly event rate VTA-; log-rank P = 0.043) were significantly lower in the VTA + cohort. At multivariate analysis, VTA was the only variable remaining associated with a lower incidence of the primary outcome [adjusted hazard ratio 0.262 (0.100-0.681), P = 0.006].
Conclusion: In a real-world registry of S-ICD carriers, the combined study endpoint of arrhythmic events and cardiovascular mortality was lower in the patient cohort undergoing VTA at long-term follow-up.
Clinicaltrials.gov identifier: NCT0473876.
Trial registration: ClinicalTrials.gov NCT00473876.
Keywords: Arrhythmic mortality; Catheter ablation; Defibrillator; Subcutaneous ICD; Ventricular tachycardia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: A.D.R. is a consultant for Abbott. M.C. has received speaker honoraria from Abbott and Biosense Webster. L.K. worked as a proctor for Boston Scientific. R.T. is a consultant for Boston Scientific, Biotronik, Biosense Webster, Abbott Medical, and he received speaker’s honoraria from Boston Scientific, Biotronik, Biosense Webster, Abbott Medical, and LifeTech and research grants from Abbott, Biosense Webster, and LifeTech. A.B. has received consultant and/or speaker fees from Abbott, Bayer Healthcare, Biosense Webster, Biotronik, Boston Scientific, Bristol Myers Squibb, Cook Medical, Daiichi Sankyo, Medtronic, Pfizer, and Spectranetics/Philips.
Figures
References
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. - PubMed
-
- Schron EB, Exner DV, Yao Q, Jenkins LS, Steinberg JS, Cook JR et al. Quality of life in the antiarrhythmics versus implantable defibrillators trial: impact of therapy and influence of adverse symptoms and defibrillator shocks. Circulation 2002;105:589–94. - PubMed
-
- Connolly SJ, Dorian P, Roberts RS, Gent M, Bailin S, Fain ES et al. Comparison of β-blockers, amiodarone plus β-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators—the OPTIC study: a randomized trial. JAMA 2006;295:165–71. - PubMed
