

Management of patients with an electrical storm or clustered ventricular arrhythmias: a clinical consensus statement of the European Heart Rhythm Association of the ESC-endorsed by the Asia-Pacific Heart Rhythm Society, Heart Rhythm Society, and Latin-American Heart Rhythm Society
- PMID: 38584423
- PMCID: PMC10999775
- DOI: 10.1093/europace/euae049
Management of patients with an electrical storm or clustered ventricular arrhythmias: a clinical consensus statement of the European Heart Rhythm Association of the ESC-endorsed by the Asia-Pacific Heart Rhythm Society, Heart Rhythm Society, and Latin-American Heart Rhythm Society
Abstract
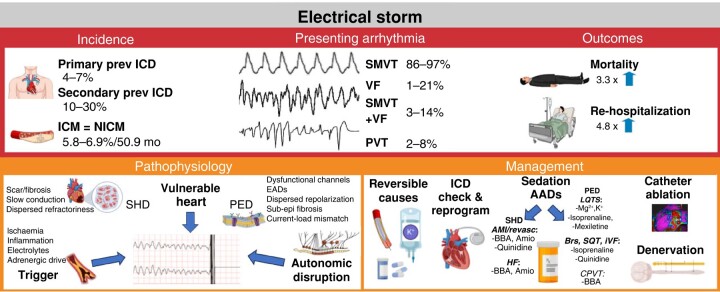
Electrical storm (ES) is a state of electrical instability, manifesting as recurrent ventricular arrhythmias (VAs) over a short period of time (three or more episodes of sustained VA within 24 h, separated by at least 5 min, requiring termination by an intervention). The clinical presentation can vary, but ES is usually a cardiac emergency. Electrical storm mainly affects patients with structural or primary electrical heart disease, often with an implantable cardioverter-defibrillator (ICD). Management of ES requires a multi-faceted approach and the involvement of multi-disciplinary teams, but despite advanced treatment and often invasive procedures, it is associated with high morbidity and mortality. With an ageing population, longer survival of heart failure patients, and an increasing number of patients with ICD, the incidence of ES is expected to increase. This European Heart Rhythm Association clinical consensus statement focuses on pathophysiology, clinical presentation, diagnostic evaluation, and acute and long-term management of patients presenting with ES or clustered VA.
Keywords: Arrhythmia; Consensus document; Electrical storm; Sudden cardiac death; Ventricular fibrillation; Ventricular tachycardia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: Radosław Lenarczyk – nothing to declare, Katja Zeppenfeld – nothing to declare, Jacob Tfelt-Hansen – support received by himself or his institution related to this work - John and Birte Meyer Family Foundation, any other financial support: Johnson and Johnson, Microport, Cytokinetics and Leo Pharma, Frank R. Heinzel – nothing to declare, Thomas Deneke speaker honoraria- Biotronik, Abbott, Biosense Webster, voted member German Cardiology Society leadership team, Elena Ene - travel and proctorship honoraria from Johnson&Johnson, Christian Meyer - Abbott: speaker, Biotronik: consultant, Biosense Webster: consultant, Boston Scientific: consultant, speaker, Arthur Wilde - Associate editor Heart Rhythm, Chair DSMB LEAP trial (unpaid), Member scientific advisory board ARMGO & ThryvTherapeutics (unpaid), Elena Arbelo - Consulting for Bayer and Biosense Webster, Ewa Jędrzejczyk-Patej – nothing to declare, Avi Sabbag – nothing to declare, Markus Stühlinger - speaker honoraria (Biotronik, Medtronic), Luigi di Biase - consultant for Biosense Webster, Stereoataxis and I-Rhythm, has received speaker honoraria/travel from Biosense Webster, St. Jude Medical (now Abbott), Boston Scientific, Medtronic, Biotronik, Atricure, Baylis and Zoll, Marmar Vaseghi – grants NIH R01HL1706262, NIH R01HL148190, honorarium for educational speaking/courses/seminars from Zoll Inc. Medtronic Inc. and Biosense Webster Inc., minor stock in NeuCures Inc, Ohad Ziv – nothing to declare, William-Fernando Bautista-Vargas – nothing to declare, Saurabh Kumar – nothing to declare, Narayanan Namboodiri – nothing to declare, Benhur Davi Henz – nothing to declare, Jose Montero Cabezas - Shockwave Inc- research funding, Penumbra Inc- speaker fees, Nikolaos Dagres – nothing to declare, Peichl Petr – Astra Zeneca, Promed, Abbott, Medtronic, Biotronik, Biosense Webster: speaker fees, consultancy, Frontera Antonio – Abbott, Boston Scientific, Biosense Webster: speaker fees, consultancy, Tzeis Stylianos – Bayer, Pfizer: speaker fees, consultancy, Merino Jose Luis – Sanofi Aventis, Microport, Medtronic, Milestone Pharmaceutical, Biotronik, Zoll Medical: speaker fees, consultancy, Bayer: travel and meeting support, Daiichi Sankyo : Clinical Trial participation, Principal investigator, Milestone : Clinical trial participation, Principal investigator, Abbott : Fellow support, Principal investigator, Medtronic : Fellow support, Principal investigator, Soejima Kyoko – Abbott, Daiichi Sankyo, Medtronic, Johnson and Johnson: speaker fees, consultancy, de Chillou Christian – Abbott, Boston Scientific, Biosense Webster: speaker fees, consultancy, Tung Roderick – Biotronik, Medtronic, Abbott: speaker fees, consultancy, Eckardt Lars - nothing to declare, Maury Philippe - nothing to declare, Hlivak Peter – Pfizer, Boehringer-Ingelheim, Bayer, Novo-Nordisk: speaker fees, consultancy, Tereshchenko Larisa - nothing to declare, Kojodjojo Pipin - nothing to declare Atie Jacob - Johnson & Johnson: speaker fees, consultancy, Boston Scientific: travel and meeting support.
Figures
References
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. - PubMed
-
- Elsokkari I, Parkash R, Tang A, Wells G, Doucette S, Yetisir E et al. Mortality risk increases with clustered ventricular arrhythmias in patients with implantable cardioverter-defibrillators. JACC Clin Electrophysiol 2020;6:327–37. - PubMed
-
- Viskin S. Long QT syndromes and torsade de pointes. Lancet 1999;354:1625–33. - PubMed
-
- Al-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society. Heart Rhythm 2018;15:e190–252. - PubMed
-
- Könemann H, Ellermann C, Zeppenfeld K, Eckardt L. Management of ventricular arrhythmias worldwide: comparison of the latest ESC, AHA/ACC/HRS, and CCS/CHRS guidelines. JACC Clin Electrophysiol 2023;9:715–28. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
