

Epidemiology of enterotoxigenic Escherichia coli and impact on the growth of children in the first two years of life in Lima, Peru
- PMID: 38584932
- PMCID: PMC10995271
- DOI: 10.3389/fpubh.2024.1332319
Epidemiology of enterotoxigenic Escherichia coli and impact on the growth of children in the first two years of life in Lima, Peru
Abstract
Background: Enterotoxigenic E. coli (ETEC) is a leading cause of diarrheal morbidity and mortality in children, although the data on disease burden, epidemiology, and impact on health at the community level are limited.
Methods: In a longitudinal birth cohort study of 345 children followed until 24 months of age in Lima, Peru, we measured ETEC burden in diarrheal and non-diarrheal samples using quantitative PCR (LT, STh, and STp toxin genes), studied epidemiology and measured anthropometry in children.
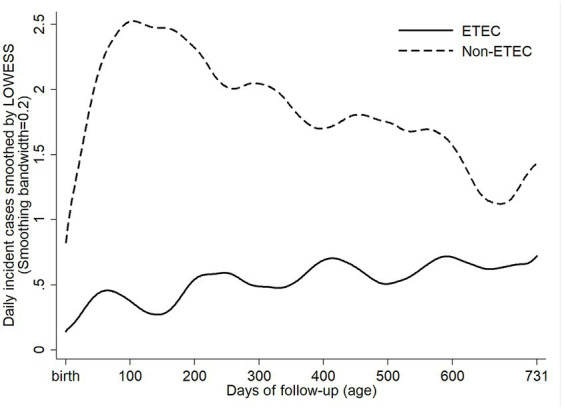
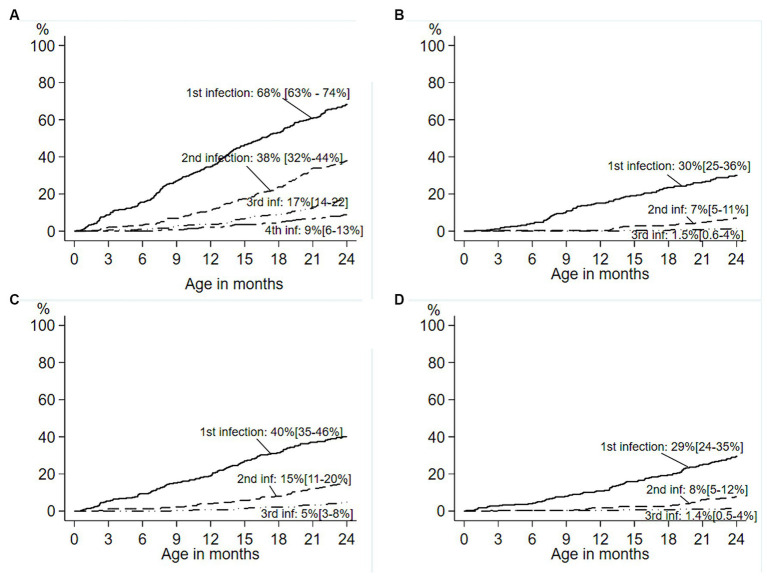
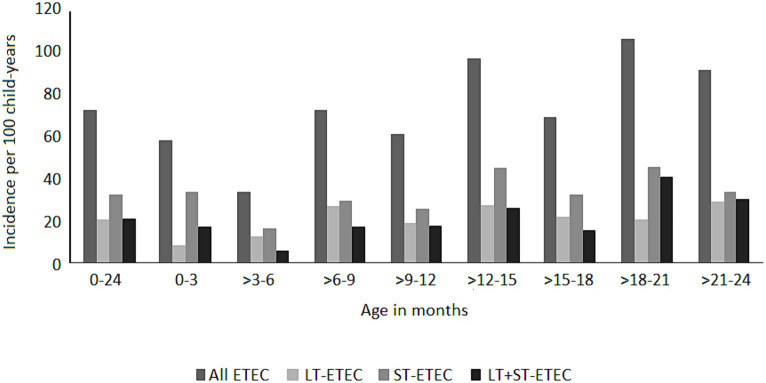
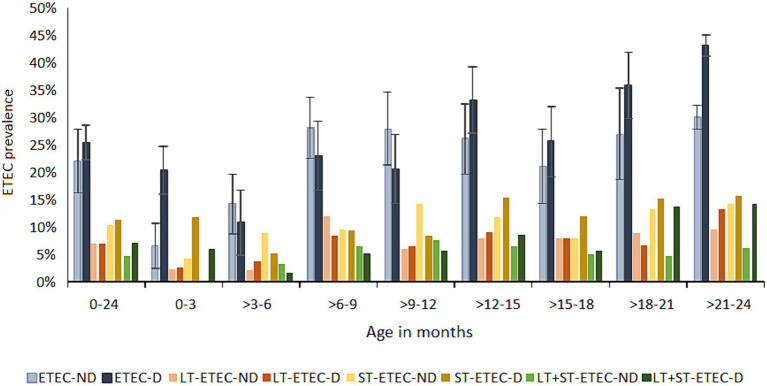
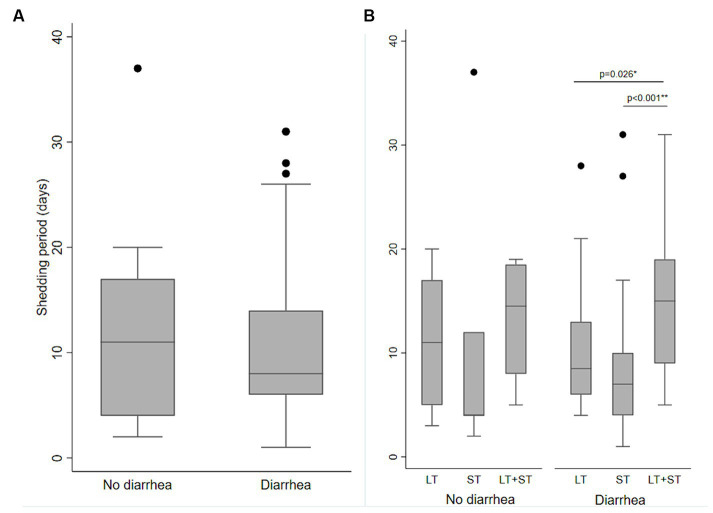
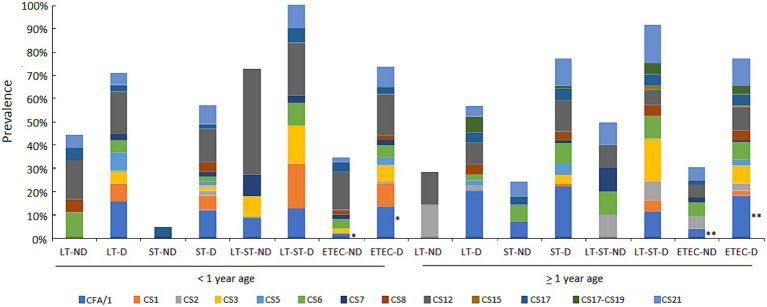
Results: About 70% of children suffered from one or more ETEC diarrhea episodes. Overall, the ETEC incidence rate (IR) was 73 per 100 child-years. ETEC infections began early after birth causing 10% (8.9-11.1) ETEC-attributable diarrheal burden at the population level (PAF) in neonates and most of the infections (58%) were attributed to ST-ETEC [PAF 7.9% (1.9-13.5)] and LT + ST-ETEC (29%) of which all the episodes were associated with diarrhea. ETEC infections increased with age, peaking at 17% PAF (4.6-27.7%; p = 0.026) at 21 to 24 months. ST-ETEC was the most prevalent type (IR 32.1) with frequent serial infections in a child. The common colonization factors in ETEC diarrhea cases were CFA/I, CS12, CS21, CS3, and CS6, while in asymptomatic ETEC cases were CS12, CS6 and CS21. Only few (5.7%) children had repeated infections with the same combination of ETEC toxin(s) and CFs, suggested genotype-specific immunity from each infection. For an average ETEC diarrhea episode of 5 days, reductions of 0.060 weight-for-length z-score (0.007 to 0.114; p = 0.027) and 0.061 weight-for-age z-score (0.015 to 0.108; p = 0.009) were noted in the following 30 days.
Conclusion: This study showed that ETEC is a significant pathogen in Peruvian children who experience serial infections with multiple age-specific pathotypes, resulting in transitory growth impairment.
Keywords: Peru; birth cohort; colonization factors; diarrhea; disease burden; enterotoxigenic E. coli; epidemiology; growth in children.
Copyright © 2024 Pajuelo, Noazin, Cabrera, Toledo, Velagic, Arias, Ochoa, Moulton, Saito, Gilman and Chakraborty.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer DS declared a shared affiliation with the author MS to the handling editor at the time of review. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- Anderson JD, Bagamian KH, Muhib F, Amaya MP, Laytner LA, Wierzba T, et al. . Burden of enterotoxigenic Escherichia coli and shigella non-fatal diarrhoeal infections in 79 low-income and lower middle-income countries: a modelling analysis. Lancet Glob Health. (2019) 7:e321–30. doi: 10.1016/S2214-109X(18)30483-2, PMID: - DOI - PMC - PubMed
-
- Kotloff KL, Nataro JP, Blackwelder WC, Nasrin D, Farag TH, Panchalingam S, et al. . Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the global enteric multicenter study, GEMS): a prospective, case-control study. Lancet. (2013) 382:209–22. doi: 10.1016/S0140-6736(13)60844-2, PMID: - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical