

Artery of Percheron Infarction: Clinical Presentation and Outcomes
- PMID: 38585441
- PMCID: PMC10996902
- DOI: 10.1212/CPJ.0000000000200266
Artery of Percheron Infarction: Clinical Presentation and Outcomes
Abstract
Background and objectives: Occlusion of the artery of Percheron (AOP) produces bilateral thalamic infarction classically leading to deficits of arousal. This nonspecific presentation complicates the diagnosis of acute ischemic stroke. We sought to describe the spectrum of clinical presentation, diagnostic neuroimaging findings, and outcomes in AOP infarction (AOPi).
Methods: We conducted a keyword search of our health system's neuroimaging database from 2014 to 2022 to identify patients with AOPi. We abstracted patient demographics, clinical presentation, neuroimaging findings, acute treatment, and modified Rankin Scale (mRS) scores (at baseline, 3 months, and 12 months). We used descriptive statistics to report our findings.
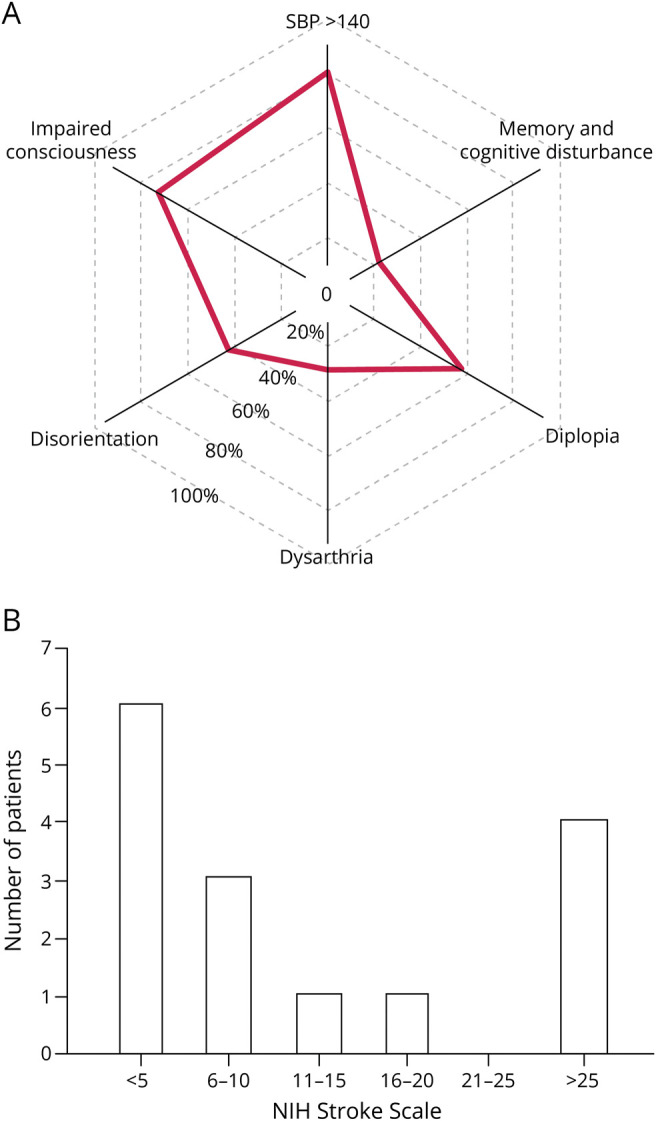
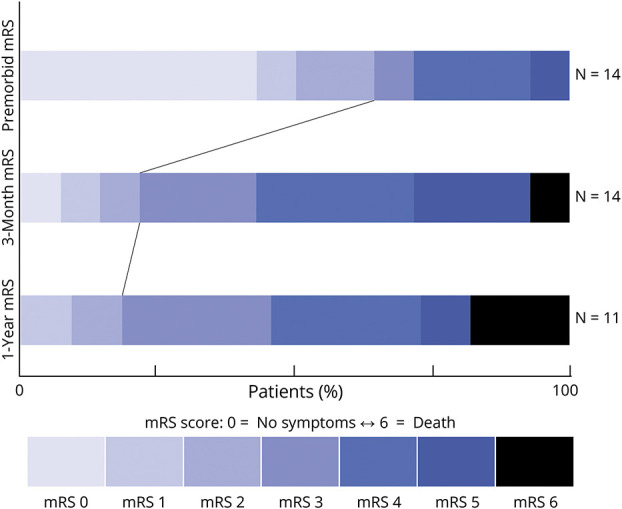
Results: Our initial keyword search identified 192 potential AOPi cases. Fifteen cases of AOPi were confirmed and included in our study (8 female [53%], median age 65 years [interquartile range (IQR): 59.5-79.5], median presenting NIHSS 6 [IQR: 2-22]). Common clinical findings on presentation were systolic blood pressure (SBP) > 140: 12 patients (80%); decreased level of consciousness (LOC): 11 patients (73%); diplopia: 8 patients (57%); disorientation: 6 patients (42%); dysarthria: 4 patients (28%); and acute memory/cognitive disturbance: 3 patients (21%). Twelve cases (80%) presented to the emergency department (ED). Median time from symptom onset to ED arrival was 774.5 minutes (IQR: 202.25-3789.0), 4 cases (27%) arrived within 4.5 hours, and one patient (7%) received intravenous thrombolysis. The median time from ED arrival to stroke diagnosis was 519.0 minutes (IQR: 227.5-1307). Head CT was only diagnostic when obtained >570 minutes from time last known well; MRI was diagnostic at all time points. Rates of functional independence (mRS ≤2) at baseline, 3 months, and 12 months were 64%, 21%, and 18%, respectively.
Discussion: The diagnosis of stroke was considerably delayed in patients with AOPi, and only one patient received IV thrombolysis. SBP >140, impaired consciousness, and diplopia were the most common findings at presentation. CT was often nondiagnostic, but MRI demonstrated bilateral thalamic infarct in all cases. AOPi caused considerable long-term morbidity. Clinicians should maintain a high degree of suspicion for AOP stroke and consider thrombolysis in appropriately selected patients.
© 2024 American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp. TAKE-HOME POINTS → The diagnosis of AOPi, a potentially disabling stroke syndrome, is often delayed, affecting acute stroke treatment.→ The findings of elevated blood pressure and diplopia in patients presenting with an acutely decreased level of consciousness can help identify patients with AOPi.→ Early, accurate diagnosis of AOPi may be facilitated by emergent MRI.
Figures

References
LinkOut - more resources
Full Text Sources