

This is a preprint.
Comprehensive genomic analysis reveals molecular heterogeneity in pediatric ALK-positive anaplastic large cell lymphoma
- PMID: 38585847
- PMCID: PMC10996813
- DOI: 10.21203/rs.3.rs-4145750/v1
Comprehensive genomic analysis reveals molecular heterogeneity in pediatric ALK-positive anaplastic large cell lymphoma
Update in
-
Comprehensive genomic analysis reveals molecular heterogeneity in pediatric ALK-positive anaplastic large cell lymphoma.Leukemia. 2025 Jan;39(1):199-210. doi: 10.1038/s41375-024-02468-4. Epub 2024 Nov 26. Leukemia. 2025. PMID: 39592809
Abstract
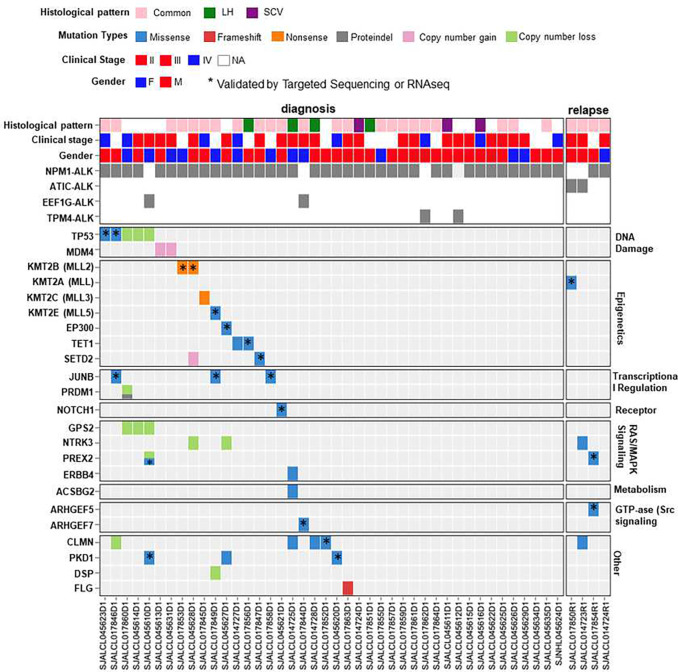
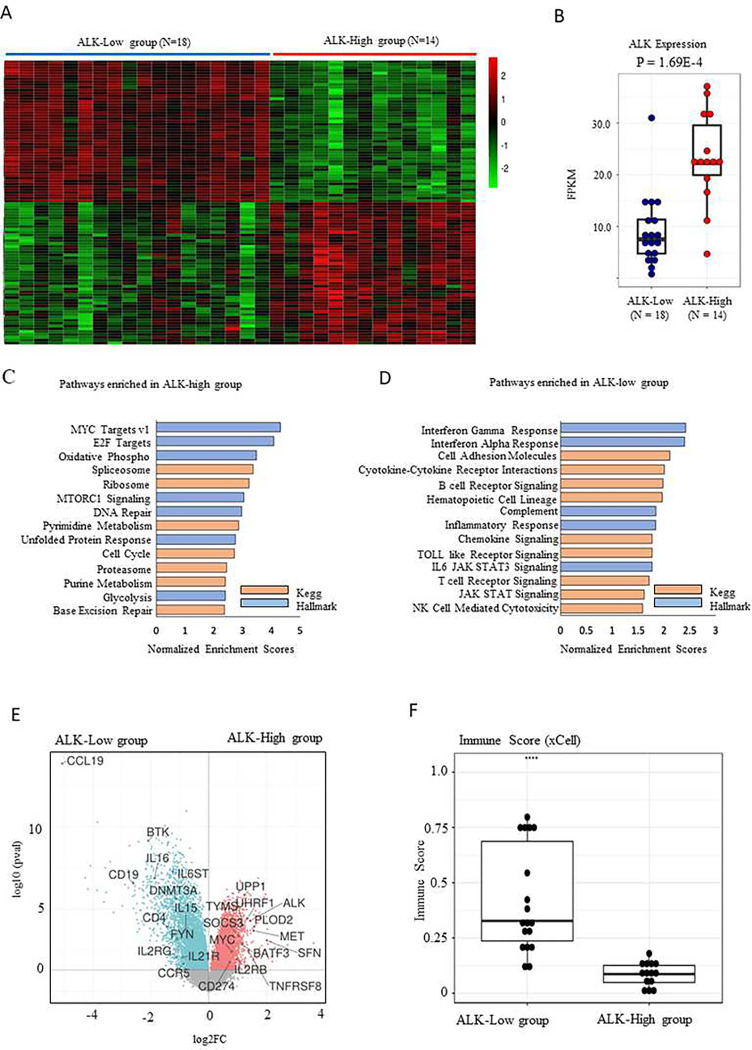
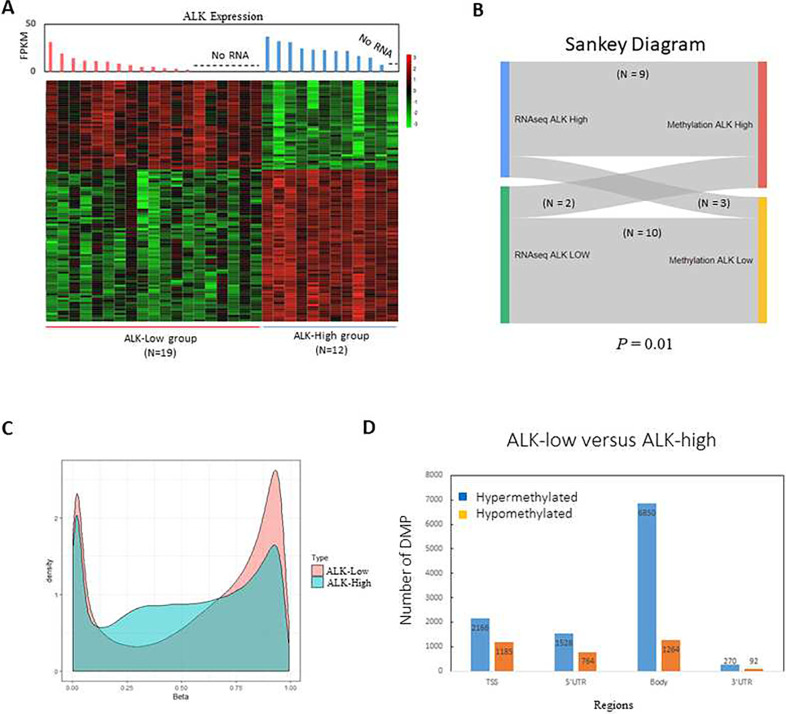
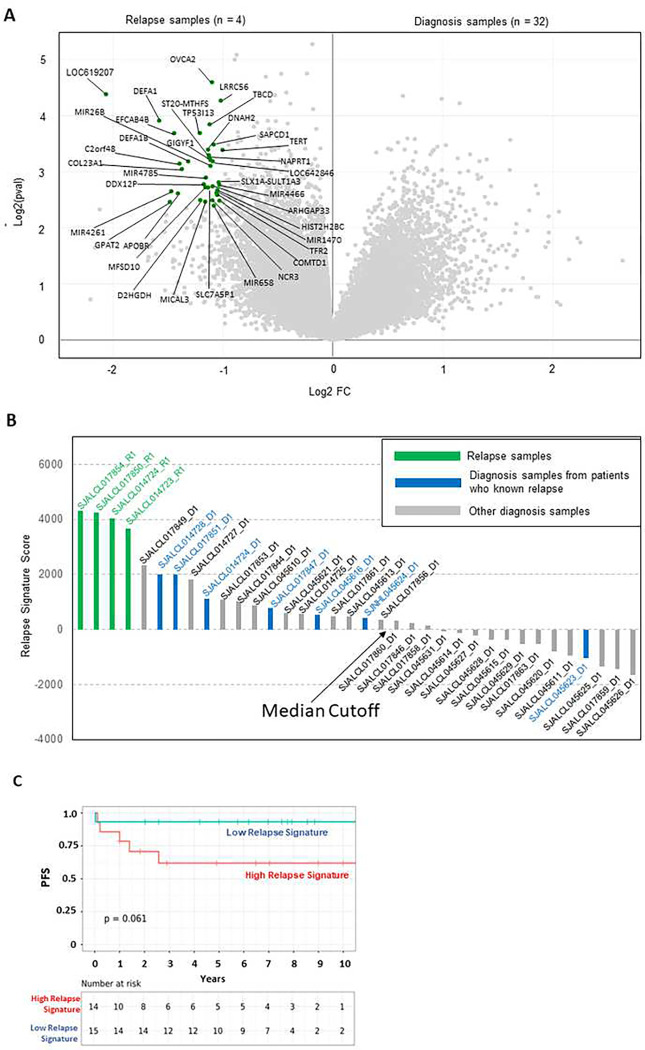
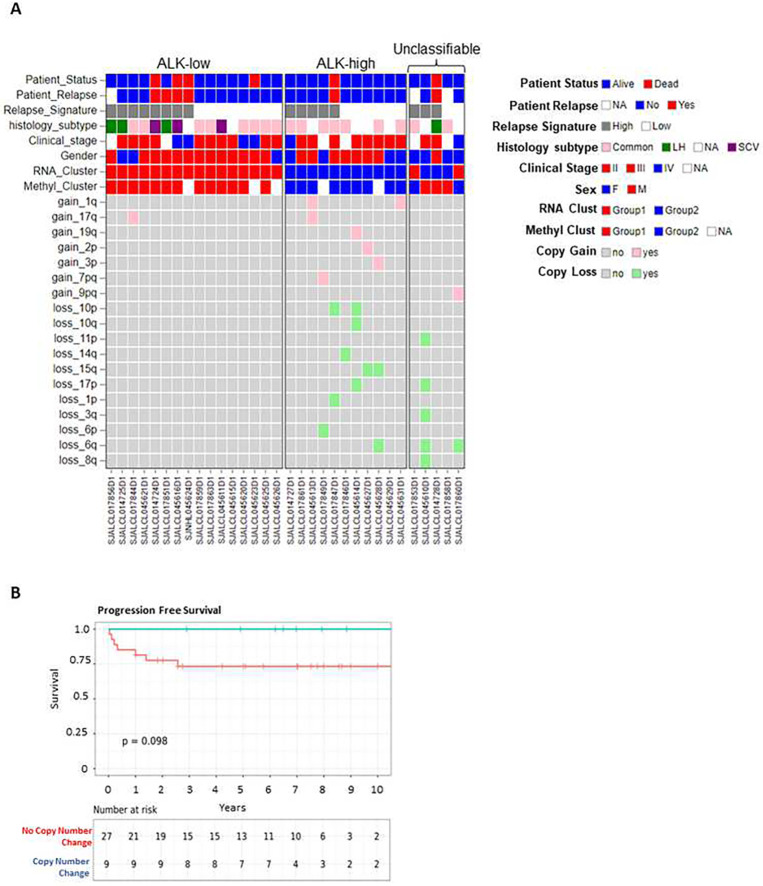
Anaplastic large cell lymphoma (ALCL) is a mature T-cell lymphoma that accounts for for 10-15% of childhood lymphomas. Despite the observation that more than 90% of pediatric cases harbor the anaplastic lymphoma kinase (ALK) rearrangement resulting in aberrant ALK kinase expression, there is significant clinical, morphologic, and biological heterogeneity. To gain insights into the genomic aberrations and molecular heterogeneity within ALK-positive ALCL(ALK+ ALCL), we analyzed 46 pediatric ALK+ ALCLs by whole-exome sequencing, RNA-sequencing, and DNA methylation profiling. Whole-exome sequencing found on average 25 SNV/Indel events per sample with recurring genetic events in regulators of DNA damage (TP53, MDM4), transcription (JUNB), and epigenetic regulators (TET1, KMT2B, KMT2A, KMT2C, KMT2E). Gene expression and methylation profiling consistently subclassified ALK+ ALCLs into two groups characterized by diferential ALK expression levels. The ALK-low group showed enrichment of pathways associated with immune response, cytokine signaling, and a hypermethylated predominant pattern compared to the ALK- high group, which had more frequent copy number changes, and was enriched with pathways associated with cell growth, proliferation, metabolic pathways, and. Taken together, these findings suggest that there is molecular heterogeneity within pediatric ALK+ALCL, predicting distinct biological mechanisms that may provide novel insights into disease pathogenesis and represent prognostic markers.
Conflict of interest statement
Conflict of Interest T.I. Shaw reports a patent for EBD CAR pending. C.G. Mullighan reports personal fees from Illumina during the conduct of the study, as well as grants from Pfizer and AbbVie, and other support from Amgen outside the submitted work. No disclosures were reported by the other authors.
Figures
References
-
- Cairo MS, Pinkerton R. Childhood, adolescent and young adult non-Hodgkin lymphoma: state of the science. Br J Haematol 2016. May 2. - PubMed
-
- Stein H, Mason DY, Gerdes J, O’Connor N, Wainscoat J, Pallesen G, et al. The expression of the Hodgkin’s disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: evidence that Reed-Sternberg cells and histiocytic malignancies are derived from activated lymphoid cells. Blood 1985. Oct; 66(4): 848–858. - PubMed
-
- Stein H, Foss HD, Durkop H, Marafioti T, Delsol G, Pulford K, et al. CD30(+) anaplastic large cell lymphoma: a review of its histopathologic, genetic, and clinical features. Blood 2000. Dec 1; 96(12): 3681–3695. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
