

Culture-Negative Neutrocytic Ascites in a Patient With Cardiac Ascites From End-Stage Heart Failure
- PMID: 38586670
- PMCID: PMC10999232
- DOI: 10.7759/cureus.55802
Culture-Negative Neutrocytic Ascites in a Patient With Cardiac Ascites From End-Stage Heart Failure
Abstract
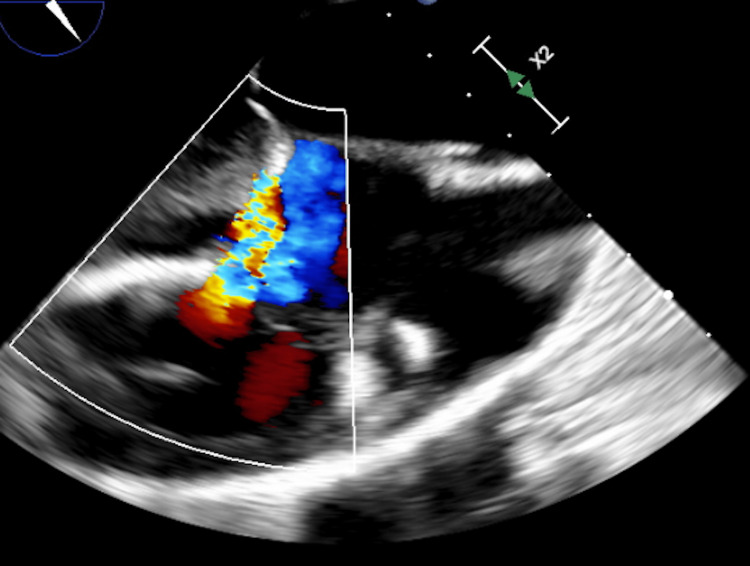
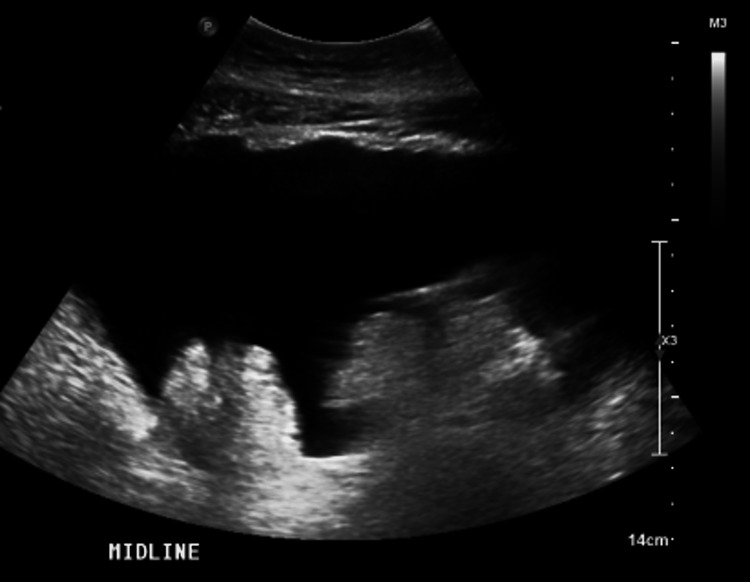
There are two significant groups of infection regarding ascitic fluid: spontaneous bacterial peritonitis (SBP) and culture-negative neutrocytic ascites (CNNA). SBP and CNNA typically occur in patients with cirrhosis. A 46-year-old male with end-stage biventricular heart failure presented with a heart failure exacerbation. He was treated with intravenous diuretics with the improvement of hypervolemia. He remained hospitalized to undergo an evaluation for tricuspid valve repair, but given the severity of his bi-ventricular heart failure, he underwent a heart transplant evaluation. As part of the work-up, he underwent an abdominal ultrasound that was significant for severe ascites but did not note an abnormal hepatic architecture suggestive of cirrhosis. A liver biopsy was then performed, which confirmed no evidence of cirrhosis. His hospitalization was complicated by refractory cardiac ascites, which required a bi-weekly paracentesis. The serum albumin-ascites gradient (SAAG) from his initial paracentesis was 1.4, indicating the etiology was from portal hypertension. The total protein was greater than 2.5 in multiple studies, so the etiology was less concerning for cirrhosis and secondary to his heart failure. About two weeks into his hospital course, he developed a leukocytosis but remained hemodynamically stable and asymptomatic from an infectious standpoint. Analysis of his ascitic fluid initially was negative for infection, but he later developed an elevated total neutrophil count on a subsequent ascitic fluid analysis study. The body fluid culture remained negative for bacterial growth. Hepatology was consulted, and he met the criteria for CNNA, so treatment with ceftriaxone was initiated. After initiating antibiotics, his leukocytosis and elevated ascitic fluid total neutrophil count resolved. Ascitic infections such as CNNA generally occur in patients with liver cirrhosis but may occur in patients without cirrhosis, as observed in our patient. This case highlights that patients with cardiac ascites can develop ascitic fluid infections that may have an impact on their mortality. The precipitating factor that enabled the patient to develop CNNA is unclear but may be related to the translocation of bacteria during his congestive heart failure exacerbation. Although uncommon in a patient with cardiac ascites, an early diagnosis of CNNA and the initiation of antibiotics can be important in preventing patient mortality.
Keywords: culture-negative neutrocytic ascities; heart failure with reduced ejection fraction; polymorphonuclear neutrophils; transesophageal echocardiogram (tee); tricuspid valve regurgitation.
Copyright © 2024, Ormachea et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Ascitic fluid infection in patients with hepatitis B virus-related liver cirrhosis: culture-negative neutrocytic ascites versus spontaneous bacterial peritonitis.J Gastroenterol Hepatol. 2010 Jan;25(1):122-8. doi: 10.1111/j.1440-1746.2009.05970.x. Epub 2009 Oct 19. J Gastroenterol Hepatol. 2010. PMID: 19845823
-
Culture-negative neutrocytic ascites: a variant of spontaneous bacterial peritonitis.Hepatology. 1984 Nov-Dec;4(6):1209-11. doi: 10.1002/hep.1840040619. Hepatology. 1984. PMID: 6500513
-
Spontaneous bacterial peritonitis and culture negative neutrocytic ascites in patients with non-alcoholic liver cirrhosis.J Gastroenterol Hepatol. 1994 Sep-Oct;9(5):433-6. doi: 10.1111/j.1440-1746.1994.tb01269.x. J Gastroenterol Hepatol. 1994. PMID: 7827291
-
Spontaneous bacterial peritonitis.Dis Mon. 1985 Sep;31(9):1-48. doi: 10.1016/0011-5029(85)90002-1. Dis Mon. 1985. PMID: 3899555 Review.
-
Does this patient have bacterial peritonitis or portal hypertension? How do I perform a paracentesis and analyze the results?JAMA. 2008 Mar 12;299(10):1166-78. doi: 10.1001/jama.299.10.1166. JAMA. 2008. PMID: 18334692 Review.
References
-
- The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites. Runyon BA, Montano AA, Akriviadis EA, Antillon MR, Irving MA, McHutchison JG. Ann Intern Med. 1992;117:215–220. - PubMed
-
- Spontaneous bacterial peritonitis and culture negative neutrocytic ascites in patients with non-alcoholic liver cirrhosis. al Amri SM, Allam AR, al Mofleh IA. J Gastroenterol Hepatol. 1994;9:433–436. - PubMed
-
- Culture-negative neutrocytic ascites: a less severe variant of spontaneous bacterial peritonitis. Pelletier G, Salmon D, Ink O, Hannoun S, Attali P, Buffet C, Etienne JP. J Hepatol. 1990;10:327–331. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous