

Minimally Invasive Vaginal Natural Orifice Transluminal Endoscopic Surgery Technique for Successful Polypropylene Mesh Removal in Pelvic Organ Prolapse: A Case Report
- PMID: 38586802
- PMCID: PMC10995651
- DOI: 10.7759/cureus.55610
Minimally Invasive Vaginal Natural Orifice Transluminal Endoscopic Surgery Technique for Successful Polypropylene Mesh Removal in Pelvic Organ Prolapse: A Case Report
Abstract
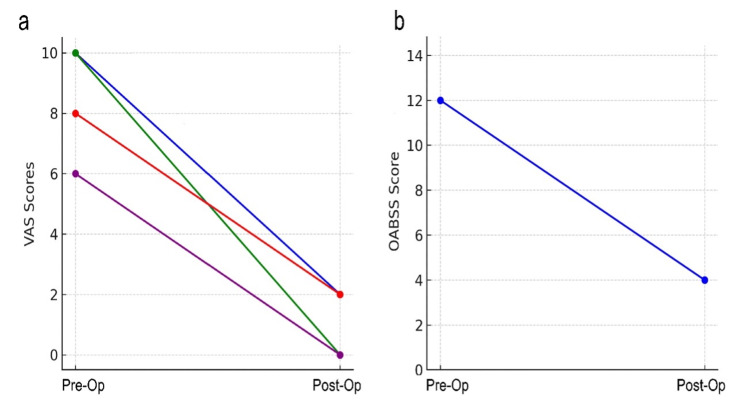
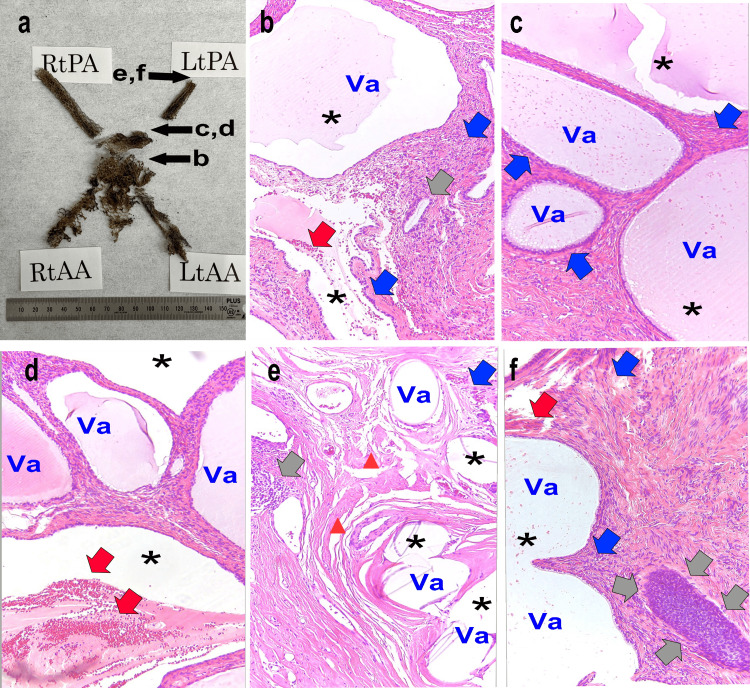
In the treatment of pelvic organ prolapse, the insertion of polypropylene mesh is often necessary but can lead to subsequent complications, such as a high incidence of pain and infections, necessitating mesh removal. However, the removal of polypropylene mesh can be challenging due to the risks of postoperative complications and technical difficulties. The key to effective healing often lies in the complete removal of the mesh, but this process is associated with complications, including severe pain and potential foreign body reactions. These challenges underscore the need for less invasive and more precise removal techniques. In our clinical practice, traditional approaches, such as vaginal and open abdominal surgeries, have often been hindered by limited visibility and accessibility at the mesh fixation sites. To address these issues, our team has pioneered the development of vaginal natural orifice transluminal endoscopic surgery (vNOTES) for mesh removal. This innovative and minimally invasive technique, performed through the vaginal route, holds particular promise for repairs within the pelvic cavity. vNOTES not only enhances surgical visibility but also reduces the invasiveness of the procedure. In this case report, we present an 85-year-old female patient, who underwent transvaginal mesh (TVM) insertion at the age of 68 years. The patient developed pain in the left buttock, left lower back, and vulvar region, necessitating the removal of TVM. The vNOTES approach significantly reduced postoperative pain and complications, enabling efficient and safe removal of the polypropylene mesh. Moreover, the pathological examination of the polypropylene mesh, which was causing hip and buttock pain, revealed the presence of poor granulation tissue, indicative of a specific pathological tissue pattern. To the best of our knowledge, this is the first detailed account of the successful application of vNOTES in mesh removal.
Keywords: mesh removal; pelvic organ prolapse; polypropylene mesh; transvaginal mesh; vaginal natural orifice transluminal endoscopic surgery; vnotes.
Copyright © 2024, Okui et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- A multicenter, randomized trial comparing pelvic organ prolapse surgical treatment with native tissue and synthetic mesh: a 5-year follow-up study. da Silveira SD, Auge AP, Jarmy-Dibella ZI, et al. Neurourol Urodyn. 2020;39:1002–1011. - PubMed
-
- Influence of polypropylene mesh degradation on tissue inflammatory reaction. Wang H, Klosterhalfen B, Klinge U, Müllen A, Jockenhoevel S. J Biomed Mater Res A. 2023;111:1110–1119. - PubMed
Publication types
LinkOut - more resources
Full Text Sources