

Medical, Surgical and Experimental Approaches to Acute Mesenteric Ischemia and Reperfusion
- PMID: 38590590
- PMCID: PMC10999141
- DOI: 10.5455/msm.2024.36.77-81
Medical, Surgical and Experimental Approaches to Acute Mesenteric Ischemia and Reperfusion
Abstract
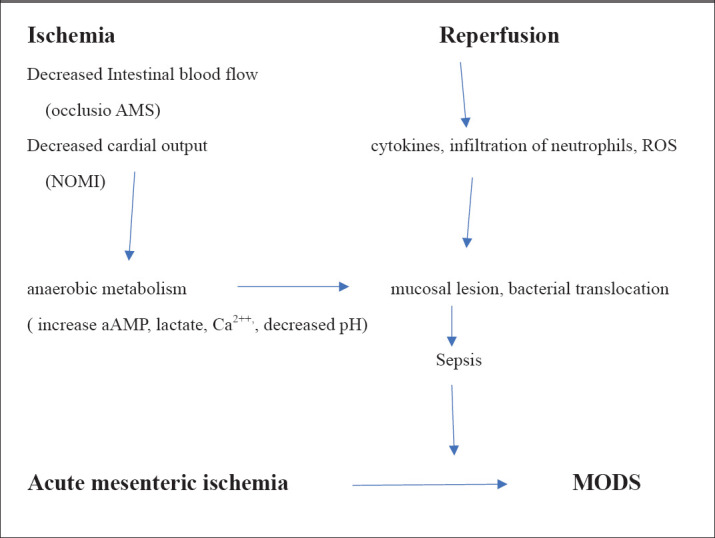
Background: Acute mesenteric ishemia(AMI) is a rare but very serious disease with high rate of mortality and morbidity. About 1-2% of all gastrointestinal disease is AMI. Mortality is about 60-80% and depends of time between starting of symptoms and establishing of diagnosis, type AMI, comorbidities. AMI is often in older population with coronary syndrom and atrial fibrilation. AMI may be occlusive(embolisatio arteriae mesentericae superior(AMS), or thrombosis of AMS, mesenterial vein thrombosis) and nonoclusive form(NOMI). NOMI is rising in critical ill patients in shock or sepsis. Pathophysiology of AMI is very complex and significant role in this proces has ischemia and also reperfusion. Reperfusion injury including oxidative stres, inflamation, infection. The best diagnostic approach is CT angiography but after high clinical suspicion on AMI. Patients have sudden, catastrophic abdominal pain, vomitus, bloody diarrhoea. Therapy is multidisciplinary-basic treatment(resuscitation with cristaloids, antibiotic, anticoagulans...), surgical treatment-resection necrotic segments of intestinum without anastomosis or endovascular treatment. In early phases conservative treatment is possible( vasodilatation, thrombolysis). In some countries there are Intestinal Stroke Centers (ISC) in which patients with AMI have better prognosis. Because of progressive nature of AMI( rapide worsening) rare are clinical study,but there are many experimental study on animal models. Most of experimental study investigate protective effects of some supstances on damage on intestinum and remote organs during ishemia and reperfusion.
Objective: To present literature data of clinical and experimental study, describe experiments on animal models and mention supstances whit promising results in protective strategies during AMI.
Methods: We analysed Pubmed by using mesh terms such as acute mesenteric ischemia, intestinal injury, reperfusion, experimental study, clinical and therapeutic approach. Results: Sudden abdominal pain resists on opioids analgetics, high rate of CRP, hyperlactatemia, increase of D dimer is enough for suspicion of AMI. Often is delayed in establishing of diagnosis of AMI. CT angiography has sensitivity of 94%. Pneumatosis is sign of necrosis of intestinal wall. Classical surgical approach is dominant, more than 70%,. Endovascular treatment became often last few years. Experimental studies investigate occlusion of AMS with atraumatic clamp, with schemia and reperfusion in different intervals Most animals models are on wistar male rats.
Conclusion: AMI has still high rate of mortality. Better diagnostic and therapeutic principles (shorter interval between appearance of symptoms and starting of therapy, multidisciplinary approach, higher percent of endovascular procedures), could decrease mortality. Experimental studies on animal models may be succesfull in development of new clinical, conservative approaches in the early phases of AMI in the future.
Keywords: acute mesenteric ischemia; experimental study; reperfusion.
© 2024 Zoran Matkovic, Zoran Aleksic.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Acosta S, Bjorck M. Modern treatment of acute mesenteric ischemia. Br J Surg. 2014 jan;101(1):e100–8. - PubMed
-
- Karkkainen KJM, Acosta S. Acute mesenteric ischemia (part I) – incidence, etiologies, and how to improve early diagnosis. Best Pract Res Clin Gastroenterol. 2017 Feb;31(1):15–25. - PubMed
-
- Kase K, Reintam Blaser A, Tamme K, Mandul M, Forbes A, Talving P, Murruste M. Epidemiology of Acute Mesenteric Ischemia.a Population-Based Investigation. World J Surg. 2023 Jan;47(1):173–181. - PubMed
-
- Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD. Acute mesenteric ischemia:a clinical review. Arch Intern Med. 2004 May 24;164(10):1054–1062. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous