

Efficacy of Alveolar Ridge Preservation in Periodontally Compromised Molar Extraction Sites: A Systematic Review and Meta-Analysis
- PMID: 38592010
- PMCID: PMC10931845
- DOI: 10.3390/jcm13051198
Efficacy of Alveolar Ridge Preservation in Periodontally Compromised Molar Extraction Sites: A Systematic Review and Meta-Analysis
Abstract
Aim: To investigate the efficacy of alveolar ridge preservation (ARP) in periodontally compromised molar extraction sites.
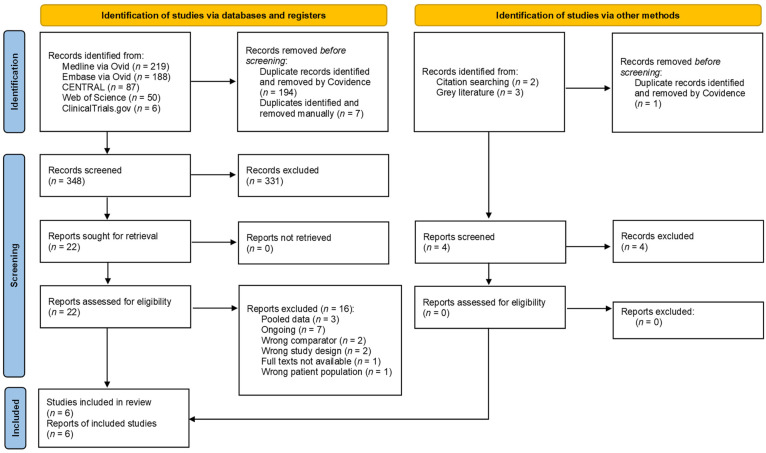
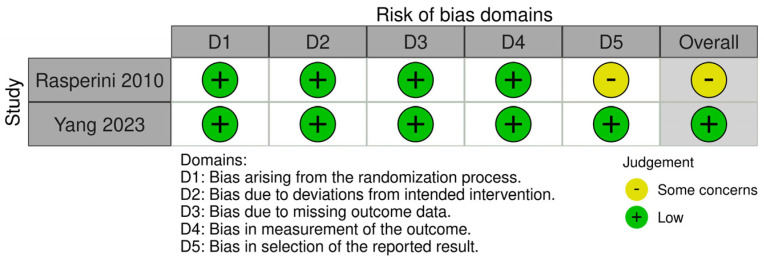
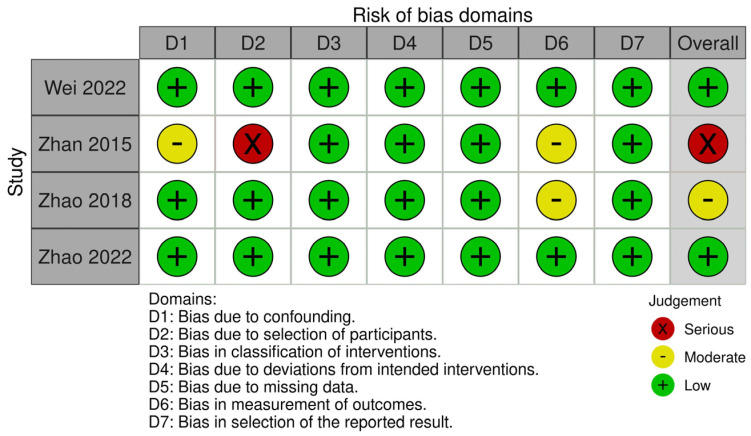
Methods: An electronic search was performed on 10th November 2023 across five databases, seeking randomised/non-randomised controlled trials (RCTs/NCTs) that included a minimum follow-up duration of four months. The RoB2 and Robins-I tools assessed the risk of bias for the included studies. Data on alveolar ridge dimensional and volumetric changes, keratinized mucosal width, and need for additional bone augmentation for implant placement were collected. Subsequently, a meta-analysis was carried out to derive the pooled estimates.
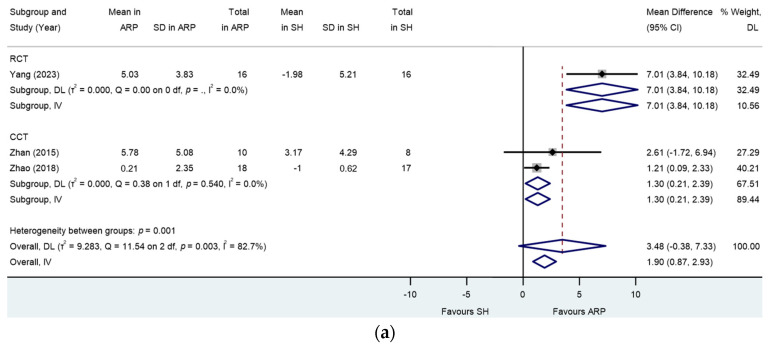
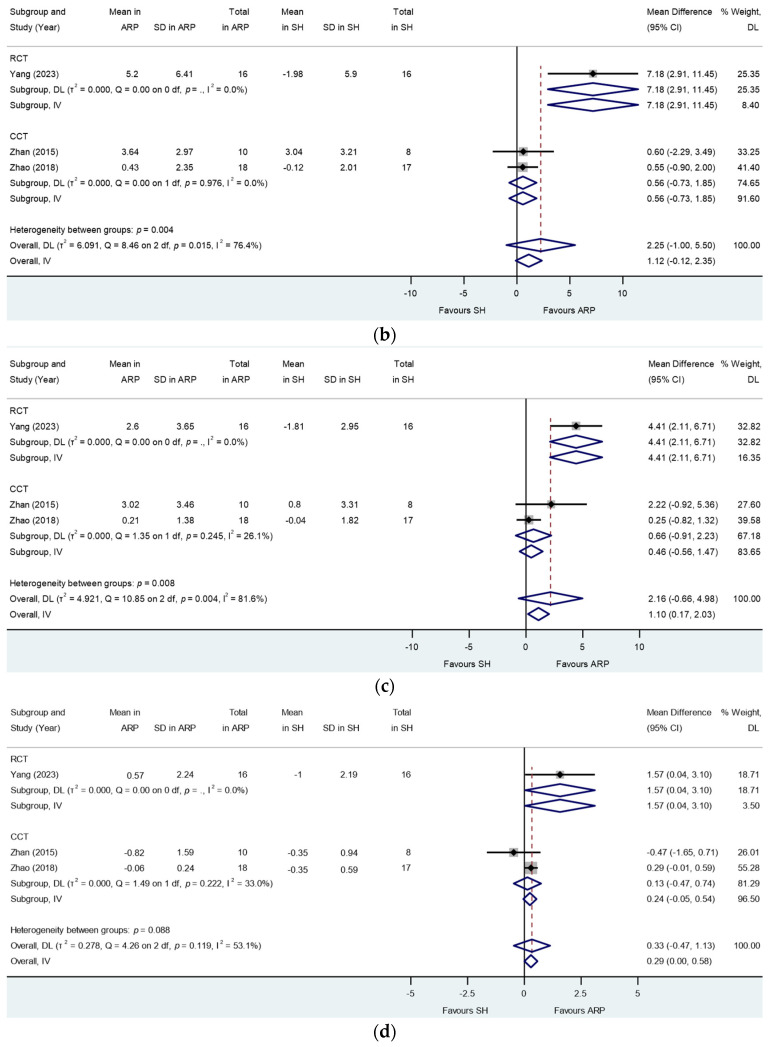
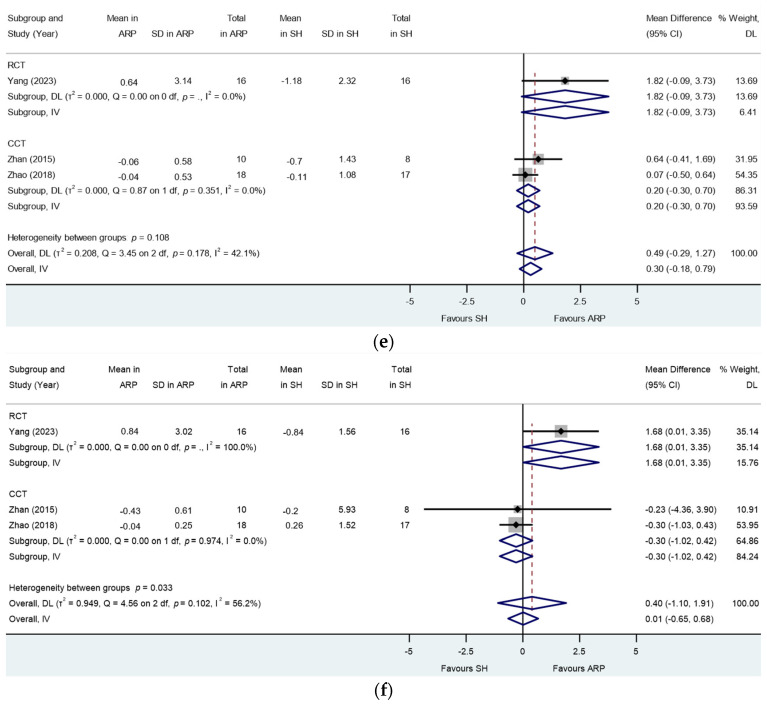
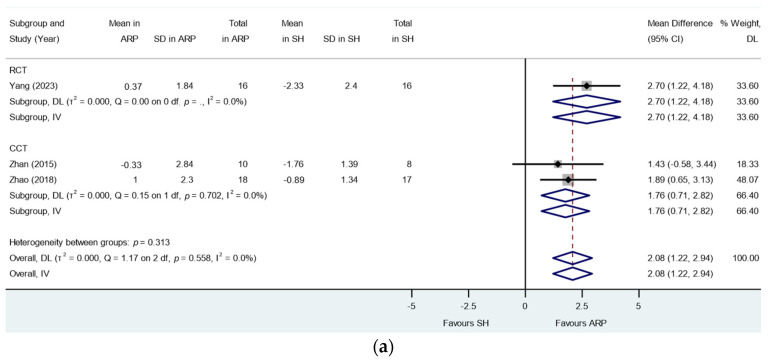
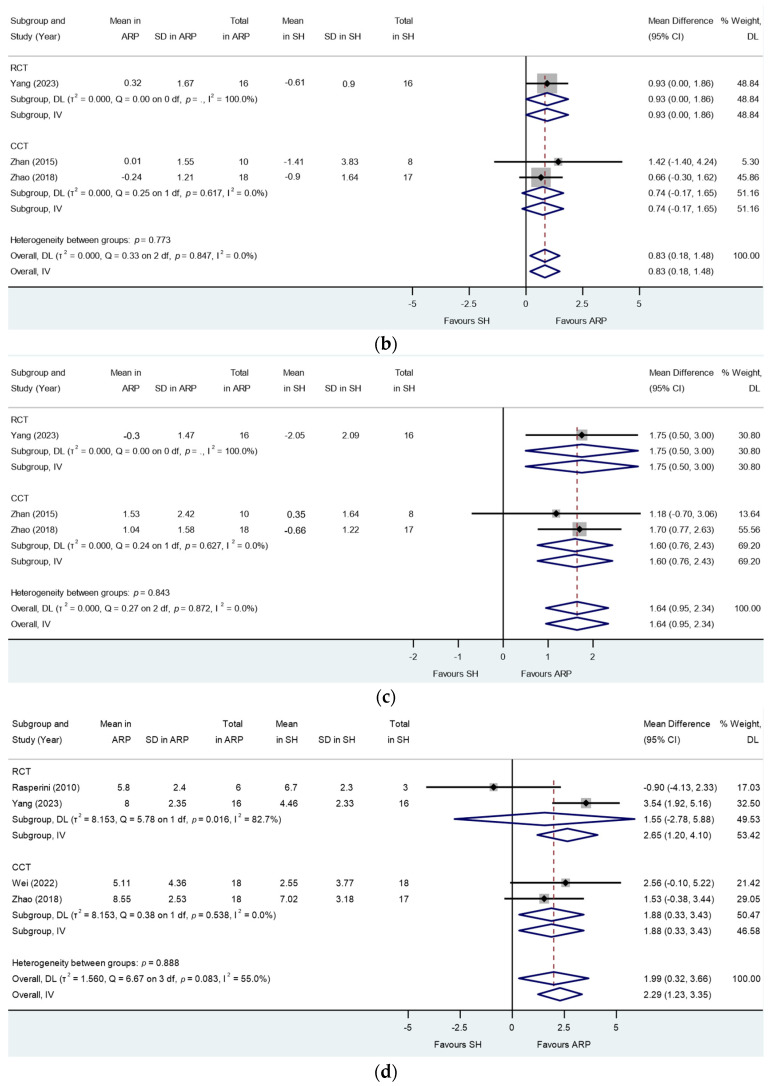
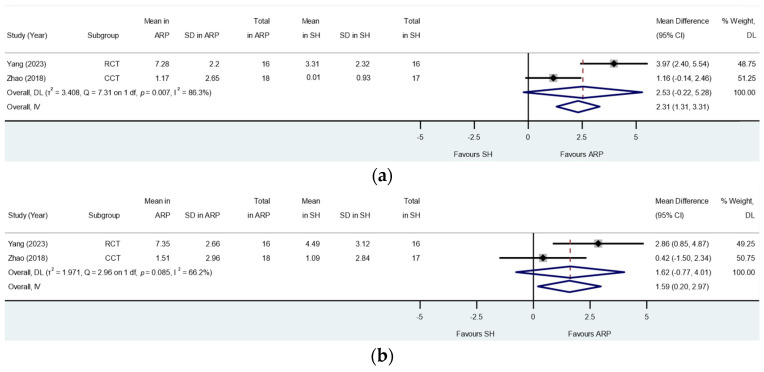
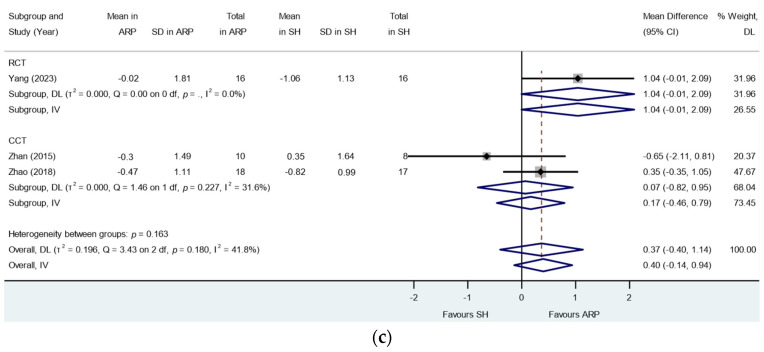
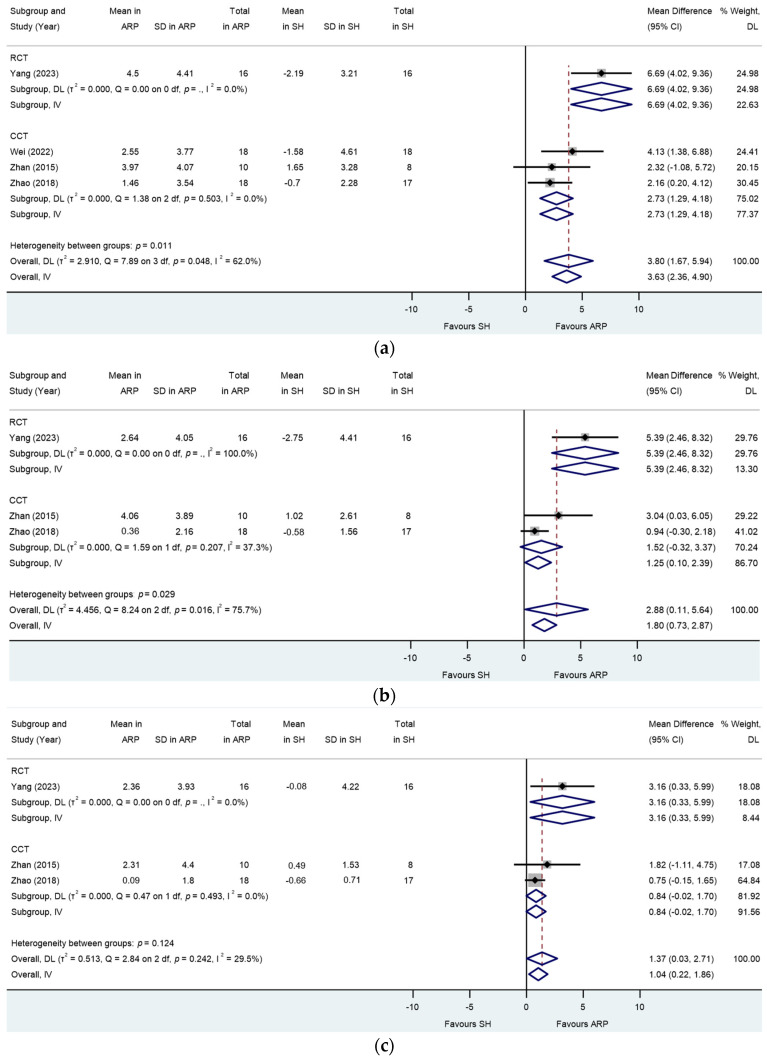
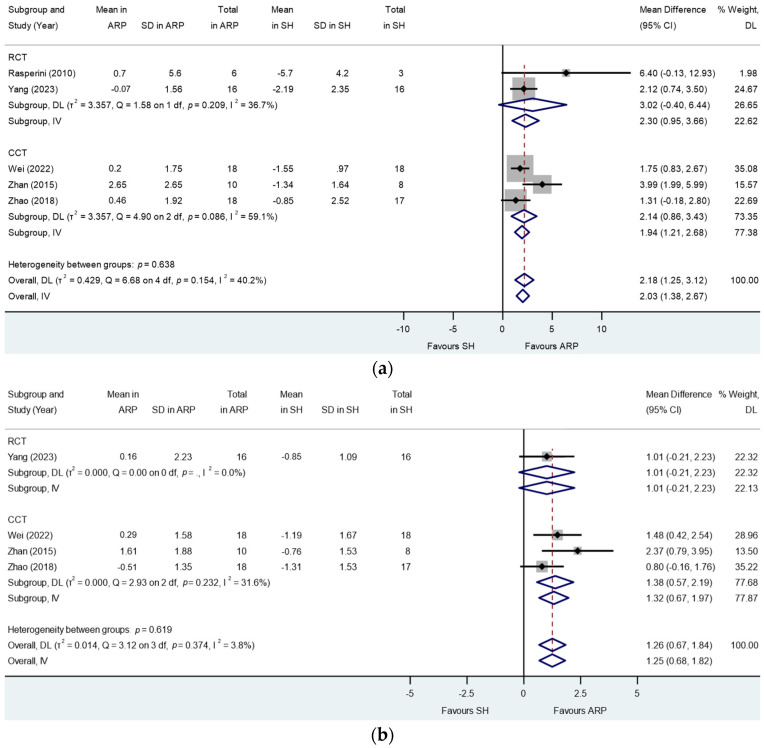
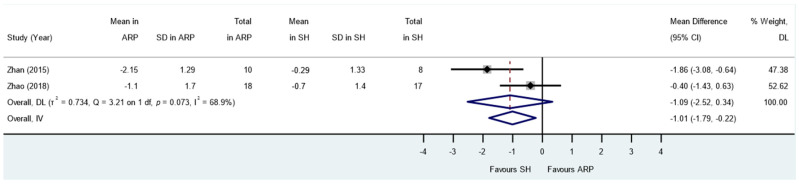
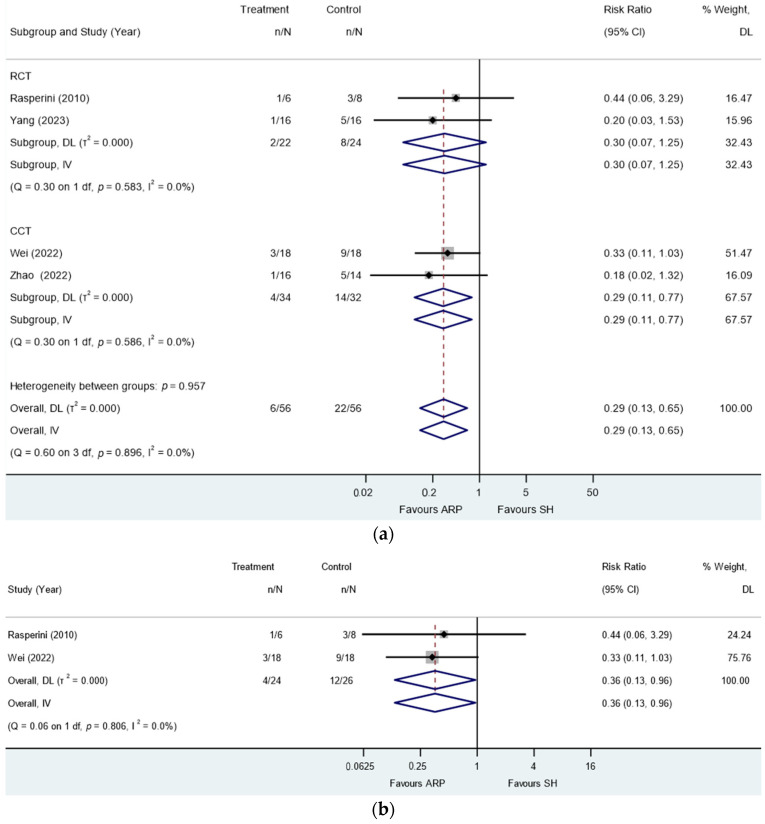
Results: Six studies were incorporated in the present review, and a total of 135 molar extraction sockets in 130 subjects were included in the meta-analysis. ARP was undertaken in 68 sites, and 67 sites healed spontaneously. The follow-up time ranged from 4 to 6 months. The meta-analysis of both RCTs and NCTs showed significant differences in mid-buccal ridge width changes at 1 mm level below ridge crest with a mean difference (MD) of 3.80 (95% CI: 1.67-5.94), mid-buccal ridge height changes (MD: 2.18; 95% CI: 1.25-3.12) and volumetric changes (MD: 263.59; 95% CI: 138.44-388.74) in favour of ARP, while the certainty of evidence is graded low to very low. Moreover, ARP appeared to reduce the need for additional sinus and bone augmentation procedures at implant placement with low certainty of evidence.
Conclusions: Within the limitations of this study, alveolar ridge preservation in periodontally compromised extraction sites may, to some extent, preserve the ridge vertically and horizontally with reference to spontaneous healing. However, it could not eliminate the need for additional augmentation for implant placement. Further, longitudinal studies with large sample sizes and refined protocols are needed.
Keywords: alveolar ridge preservation; extraction; molar; periodontally compromised; periodontitis; systematic review.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Fok M.R., Pelekos G., Tonetti M.S. Feasibility and needs for simultaneous or staged bone augmentation to place prosthetically guided dental implants after extraction or exfoliation of first molars due to severe periodontitis. J. Clin. Periodontol. 2020;47:1237–1247. doi: 10.1111/jcpe.13344. - DOI - PubMed
-
- Rasperini G., Canullo L., Dellavia C., Pellegrini G., Simion M. Socket grafting in the posterior maxilla reduces the need for sinus augmentation. Int. J. Periodontics Restor. Dent. 2010;30:265–273. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
